
Aortic Dissection: The Tearing Chest Pain Emergency You Must Not Miss
Some medical emergencies announce themselves loudly and unmistakably. Aortic dissection is one of them. Patients and doctors who have witnessed it frequently describe the pain as the worst imaginable — sudden, tearing, and ripping through the chest or back with catastrophic intensity.
Yet despite its dramatic presentation, aortic dissection is frequently misdiagnosed. Every minute without treatment raises the risk of death. Understanding this condition — its warning signs, its causes, and why it demands immediate emergency care — could mean the difference between life and death.
What Is Aortic Dissection?
The aorta is the largest artery in the human body. It carries oxygen-rich blood directly from the heart, arching upward and then descending through the chest and abdomen to supply the entire body. The aortic wall consists of three distinct layers — the intima (inner), media (middle), and adventitia (outer).
How the Tear Happens
Aortic dissection occurs when a tear develops in the inner layer of the aortic wall. Blood surges through this tear under high pressure, separating the inner and middle layers and creating a false channel alongside the true aortic channel. This separation, called dissection, can extend rapidly along the length of the aorta in either direction.
The false channel created by the dissection competes with the true channel for blood flow. Organs that depend on branches arising from the dissected segment can lose their blood supply entirely. This is why aortic dissection causes not only severe pain but also strokes, heart attacks, kidney failure, and limb ischaemia simultaneously.
How Common Is Aortic Dissection?
Aortic dissection affects approximately 3 in every 100,000 people per year. Though relatively uncommon, its high mortality without treatment makes it one of the most feared cardiovascular emergencies. Historically, untreated Type A aortic dissection — the most dangerous form — carries a mortality rate of approximately 1–2% per hour in the first 48 hours after symptom onset.
Who It Affects
Aortic dissection predominantly affects people between 60 and 80 years of age, though it can occur at any age. Men develop aortic dissection approximately two to three times more often than women. However, women tend to present later, receive less timely diagnosis, and experience higher in-hospital mortality — a disparity that highlights the urgent need for greater awareness across all demographics.
Types of Aortic Dissection
Doctors classify aortic dissection using two primary systems: the Stanford and DeBakey classifications. Understanding these classifications is important because they directly determine treatment.
Stanford Classification
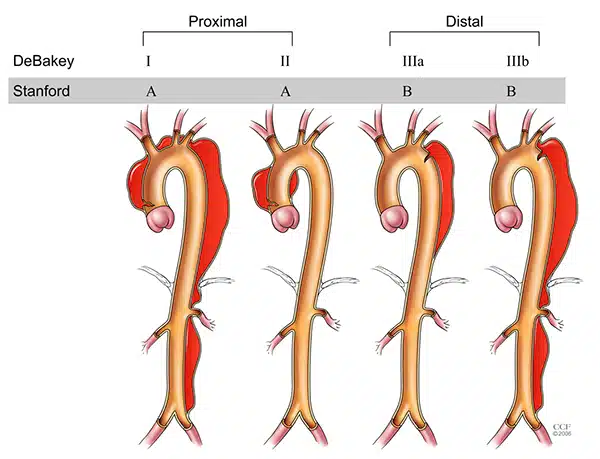
The Stanford system divides aortic dissection into two types. Stanford Type A involves the ascending aorta — the portion of the aorta closest to the heart — regardless of where the tear originates. Stanford Type B involves only the descending aorta, beginning beyond the origin of the left subclavian artery supplying the left arm.
Type A dissection is the more dangerous form. It threatens the heart itself, can block the coronary arteries, and may cause the aortic valve to leak. Type A dissection demands emergency open-heart surgery.
Stanford Type B Dissection
Type B dissection, involving only the descending aorta, generally carries a lower immediate mortality than Type A. Many uncomplicated Type B dissections respond to aggressive medical management — primarily intensive blood pressure control. However, complicated Type B dissection, involving organ ischaemia, rapid expansion, or rupture, typically requires endovascular stent grafting or open surgical repair.
The DeBakey Classification
The DeBakey system offers a more granular classification into three types based on the origin and extent of the dissection. Type I involves the entire aorta from ascending to descending. Type II affects only the ascending aorta. Type III involves only the descending aorta and corresponds broadly to Stanford Type B. In daily clinical practice, the Stanford classification is more widely used due to its direct treatment implications.
What Causes Aortic Dissection?
Aortic dissection results from structural weakening of the aortic wall, usually combined with haemodynamic stress from elevated blood pressure. Several conditions and risk factors predispose the aortic wall to this catastrophic failure.
High Blood Pressure
Hypertension — chronically elevated blood pressure — is the single most important risk factor for aortic dissection. Sustained high blood pressure exerts relentless mechanical stress on the aortic wall. Over years, this stress progressively weakens the structural integrity of the wall’s middle layer, setting the stage for dissection.
Approximately 70% of people who develop aortic dissection have a history of hypertension. Poorly controlled blood pressure substantially increases risk compared to well-managed hypertension.
Inherited Connective Tissue Disorders
Genetic conditions that weaken connective tissue — the structural scaffolding of blood vessel walls — significantly elevate the risk of aortic dissection, often at a younger age. Marfan syndrome causes mutations in the fibrillin-1 gene, leading to aortic dilation and increased dissection risk. People with Marfan syndrome often have tall stature, long limbs, lens dislocation, and cardiac abnormalities.
Ehlers-Danlos syndrome (vascular type), Loeys-Dietz syndrome, and Turner syndrome also carry elevated aortic dissection risk. Genetic counselling and regular aortic surveillance imaging are essential for affected individuals and their families.
Bicuspid Aortic Valve
A bicuspid aortic valve — a congenital abnormality where the aortic valve has two leaflets instead of the normal three — is present in approximately 1–2% of the population. This abnormality is associated with structural aortic wall weakness and progressive aortic dilation that increases dissection risk over time. Regular imaging surveillance identifies those who require prophylactic surgical repair before dissection occurs.
Other Risk Factors
Aortic aneurysm — abnormal dilation of the aorta — predisposes to dissection. Cocaine and amphetamine use cause acute, dramatic spikes in blood pressure that can precipitate dissection even in young people without pre-existing aortic disease. Pregnancy, particularly in the third trimester and peripartum period, increases dissection risk in women with underlying aortic conditions.
Chest trauma from high-speed vehicle accidents, previous cardiac surgery, and certain inflammatory aortic conditions such as giant cell arteritis round out the major risk factors.
Recognising the Symptoms
Aortic dissection produces a constellation of symptoms that is both characteristic and highly variable. Recognising the hallmark presentation is critical, as diagnostic delays worsen outcomes dramatically.
The Classic Tearing Pain
Sudden, severe chest or back pain is the defining symptom of aortic dissection. Patients and witnesses consistently describe this pain as tearing, ripping, or knife-like in quality. It typically reaches maximum intensity immediately at onset — unlike the crescendo pain of heart attack, which builds gradually over minutes.
The location of pain provides clues about the dissection type. Anterior chest pain suggests ascending aortic involvement. Pain radiating to the back, between the shoulder blades, points toward descending aortic dissection. Pain that migrates downward toward the abdomen or legs suggests extension of the dissection along the aorta.
Symptoms From Branch Vessel Involvement
As the dissection extends and compromises blood flow to branch arteries, additional symptoms emerge based on which organs lose perfusion. Stroke symptoms — facial drooping, arm weakness, speech difficulty — indicate carotid artery involvement. Acute limb pain, pallor, and pulselessness signal disruption of arterial supply to the arms or legs.
Acute kidney failure, severe abdominal pain from gut ischaemia, and paraplegia from spinal cord ischaemia can all occur when dissection interrupts key arterial branches. This constellation of seemingly unrelated symptoms arising simultaneously is a crucial clue pointing toward aortic catastrophe.
Cardiovascular Collapse
Type A aortic dissection can cause acute aortic valve regurgitation — severe leaking of the aortic valve — leading to acute heart failure and cardiogenic shock. When the dissection extends into the coronary arteries, it triggers a simultaneous heart attack. Haemopericardium — blood filling the pericardial sac — causes cardiac tamponade, a rapidly fatal compression of the heart that collapses blood pressure and circulation.
Symptoms That Can Mislead
Aortic dissection mimics other serious conditions, which partly explains diagnostic delays. Patients may present with syncope (fainting), pulse deficits between arms, hypertension in one arm and hypotension in the other, or a new aortic regurgitation murmur. Recognising these atypical features alongside the classic tearing pain pattern sharpens clinical suspicion significantly.
How Doctors Diagnose Aortic Dissection
Diagnosing aortic dissection combines clinical suspicion, rapid bedside assessment, and urgent imaging. Speed is paramount — every minute matters.
Clinical Assessment and Risk Scores
Emergency physicians use structured risk assessment tools such as the Aortic Dissection Detection Risk Score (ADD-RS) to stratify clinical suspicion rapidly. Factors such as the nature of pain, presence of pulse deficits, blood pressure difference between arms, known aortic disease, and predisposing conditions all contribute to the clinical risk calculation.
High clinical suspicion demands immediate imaging without delay for further bedside investigations.
D-Dimer Blood Test
A highly sensitive D-dimer blood test — measuring a protein fragment produced when blood clots break down — can help rule out aortic dissection when clinical suspicion is low and the result is negative. However, a positive D-dimer is non-specific and does not confirm dissection. Critically, a negative D-dimer in a high-suspicion patient does not exclude dissection and should not delay imaging.
CT Aortography
CT aortography — a contrast-enhanced CT scan of the aorta — is the diagnostic gold standard for aortic dissection in most emergency settings. It visualises the entire aorta rapidly, identifies the extent of dissection, detects branch vessel involvement, and guides surgical or endovascular planning. Modern CT scanners can complete this scan within minutes.
CT aortography identifies the intimal flap — the torn inner layer visible as a membrane dividing the true and false channels — with exquisite clarity. It also detects haemopericardium, aortic aneurysm size, and branch vessel compromise.
Transoesophageal Echocardiography
Transoesophageal echocardiography (TOE) provides detailed real-time imaging of the heart and ascending aorta. It is particularly valuable in haemodynamically unstable patients who cannot safely undergo CT scanning. TOE can confirm Type A dissection, assess aortic valve function, and detect pericardial effusion rapidly at the bedside.
MRI and Chest X-Ray
MRI offers excellent aortic imaging without radiation but takes significantly longer than CT and is impractical in emergencies. Chest X-ray may show a widened mediastinum — the central chest compartment containing the aorta — in some cases of aortic dissection, but a normal X-ray does not exclude dissection. Clinicians use chest X-ray as a rapid initial screen while organising definitive imaging.
Emergency Treatment of Aortic Dissection
Treatment depends on dissection type, extent, and the presence of complications. Both Type A and Type B dissection require immediate admission to a specialist centre with aortic surgery capability.
Medical Stabilisation
Regardless of dissection type, the immediate priority is reducing blood pressure and heart rate to limit the propagation of the tear. Intravenous beta-blockers — particularly esmolol or labetalol — lower both blood pressure and the rate of pressure change within the aorta with each heartbeat. Target blood pressure is typically below 120 mmHg systolic, achieved rapidly and maintained consistently.
Adequate intravenous analgesia is equally important. Controlling pain reduces sympathetic nervous system activation, which itself drives blood pressure elevation.
Emergency Surgery for Type A Dissection
Type A aortic dissection requires emergency open-heart surgery to prevent death from cardiac tamponade, acute aortic regurgitation, or coronary artery involvement. Surgeons replace the torn ascending aorta with a synthetic graft, repair or replace the aortic valve if necessary, and restore normal coronary blood flow.
Surgery for Type A dissection carries significant risk, but this risk is far lower than the near-certain mortality of untreated dissection. Outcomes continue to improve as aortic centres accumulate experience and refine surgical techniques.
Endovascular Treatment for Type B Dissection
Thoracic endovascular aortic repair (TEVAR) — placing a stent graft inside the aorta via a catheter through the groin — has transformed the management of complicated Type B dissection. TEVAR seals the entry tear, redirects blood flow into the true channel, and prevents rupture without requiring open chest surgery.
Uncomplicated Type B dissection typically receives intensive medical therapy alone, with close imaging surveillance. Surgery is reserved for complications including malperfusion, rapid aortic expansion, persistent pain, or haemodynamic instability despite medication.
Surviving Aortic Dissection: Recovery and Long-Term Care
Surviving aortic dissection is a significant achievement, but recovery requires lifelong commitment to monitoring and risk factor management.
Immediate Post-Operative Recovery
Recovery from Type A surgical repair involves time in intensive care, careful haemodynamic monitoring, and management of post-operative complications including bleeding, stroke, and renal impairment. Most patients spend several days in intensive care before transfer to a cardiac surgery ward. Full recovery from surgery typically takes several weeks to months.
Lifelong Blood Pressure Control
Regardless of treatment type, all survivors of aortic dissection require meticulous lifelong blood pressure control. Target blood pressure is generally below 130/80 mmHg, achievable with medications including beta-blockers, ACE inhibitors, and calcium channel blockers. Regular home blood pressure monitoring empowers patients to maintain optimal control between clinic visits.
Surveillance Imaging
Regular CT or MRI aortic surveillance is essential for detecting late complications including false channel expansion, aneurysm formation, and extension of dissection. Imaging is typically performed at one month, six months, and twelve months after the acute event, then annually if stable. Patients with connective tissue disorders require even closer surveillance.
Activity and Lifestyle Adjustments
Aortic dissection survivors should avoid isometric exercises — activities involving sustained muscle contraction against resistance, such as heavy weightlifting — as these cause sharp blood pressure spikes. Moderate aerobic exercise, smoking cessation, dietary sodium reduction, and healthy weight maintenance all support long-term aortic health. A cardiac rehabilitation programme provides structured, supervised guidance on safe return to activity.
Frequently Asked Questions
How is aortic dissection different from a heart attack?
Aortic dissection and heart attack both cause severe chest pain and can occur together, but they are distinct conditions. A heart attack results from blocked coronary arteries cutting off blood supply to the heart muscle. Aortic dissection involves a tear in the aortic wall that creates a false channel and threatens multiple organs simultaneously. The pain character differs — heart attack pain typically builds gradually, while aortic dissection pain strikes instantly at maximum severity.
Can aortic dissection be prevented?
While not all cases are preventable, managing key risk factors significantly reduces individual risk. Treating high blood pressure consistently and effectively is the most impactful preventive measure. People with inherited connective tissue disorders, bicuspid aortic valves, or a family history of aortic disease should undergo regular aortic imaging surveillance and consider prophylactic surgical repair if the aorta reaches concerning dimensions.
What is the survival rate for aortic dissection?
Survival depends heavily on dissection type and speed of treatment. Without surgery, Type A aortic dissection carries a mortality rate of approximately 1–2% per hour, meaning half of untreated patients die within 48 hours. With prompt surgical intervention at an experienced centre, in-hospital survival rates for Type A dissection reach approximately 70–85%. Uncomplicated Type B dissection managed medically has a much better short-term prognosis, with in-hospital mortality below 10%.
Is aortic dissection hereditary?
Aortic dissection is not directly hereditary in most cases, but certain underlying genetic conditions that predispose to it are inherited. Marfan syndrome, Loeys-Dietz syndrome, and vascular Ehlers-Danlos syndrome all follow inheritance patterns and significantly elevate family members’ risk. Anyone with a first-degree relative diagnosed with aortic dissection or aortic aneurysm should discuss screening with their doctor.
Why does aortic dissection sometimes go undiagnosed?
Aortic dissection can mimic heart attack, pulmonary embolism, stroke, and musculoskeletal chest pain, leading to diagnostic confusion. Atypical presentations — including syncope, abdominal pain, or neurological symptoms without prominent chest pain — further complicate recognition. The consequences of misdiagnosis are severe, as administering blood thinners intended for heart attack treatment can be catastrophic in aortic dissection.
Can someone live a normal life after aortic dissection?
Many survivors of aortic dissection lead meaningful, active lives following appropriate treatment and recovery. Lifelong blood pressure management, regular surveillance imaging, and activity modifications are necessary components of long-term care. Psychological recovery is also important, as many survivors experience anxiety and post-traumatic stress. Cardiac rehabilitation and mental health support both contribute meaningfully to quality of life after aortic dissection.
Conclusion
Aortic dissection is one of cardiovascular medicine’s most dramatic and unforgiving emergencies. Its sudden onset, rapidly fatal trajectory, and capacity to mimic other conditions make it both terrifying and critically important to recognise. The characteristic tearing chest or back pain that reaches peak intensity immediately must never be dismissed or delayed.
Advances in CT imaging, endovascular surgery, and specialist aortic centres have transformed survival rates over recent decades. Yet awareness remains the most powerful first link in the survival chain. If someone experiences sudden, severe, tearing chest or back pain — especially with known risk factors — they need emergency care immediately. Act fast, and the aorta can be saved.
References
- Marfan syndrome is caused by mutations in the FBN1 gene located on chromosome 15.
- The aortic valve sits between the left ventricle and the aorta, the body’s largest artery.
- Ehlers-Danlos syndrome is a heterogeneous group of genetic connective tissue disorders caused by collagen defects characterized by joint hypermobility,
- Turner syndrome is a genetic condition affecting females where one of the two X chromosomes is completely or partially missing.
Disclaimer:
This article is for general informational purposes only and does not constitute medical advice. Always seek immediate emergency care for sudden severe chest or back pain. Consult a qualified healthcare professional for personalised medical guidance.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.