
Aortic Stenosis: Why This Heart Valve Condition Is Increasingly Common in Older Adults
Aortic Stenosis is a serious and increasingly prevalent heart valve condition in which the aortic valve narrows progressively, obstructing blood flow from the heart to the rest of the body. The aortic valve acts as the heart’s main exit gate, opening with each heartbeat to allow oxygen-rich blood to pass from the left ventricle into the aorta and onward to every organ in the body. When this valve stiffens and narrows, the heart must work dramatically harder to push blood through the reduced opening.
What makes Aortic Stenosis particularly important today is its strong association with ageing. As populations worldwide grow older, the number of people developing this condition is rising sharply. Once symptoms appear, survival without treatment drops precipitously. Yet modern interventional cardiology has transformed the outlook, offering minimally invasive options that can restore quality and length of life even in the most elderly and frail patients. Understanding Aortic Stenosis thoroughly has never been more clinically relevant.
What Is Aortic Stenosis?
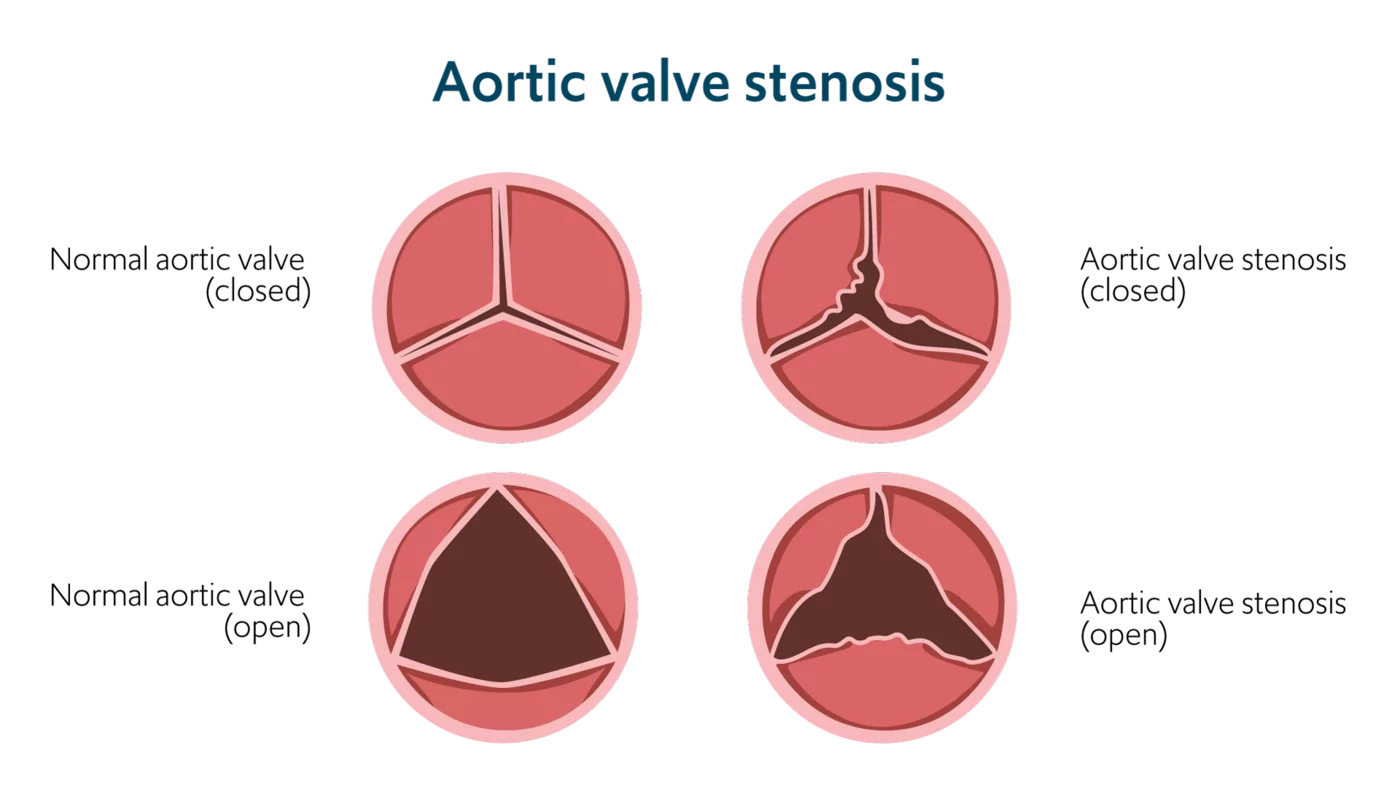
The aortic valve sits between the left ventricle and the aorta, the body’s largest artery. Normally, this valve opens fully with each contraction of the left ventricle, allowing unobstructed blood flow. In Aortic Stenosis, the valve leaflets, the flaps that open and close, become thickened, calcified, and rigid over time.
This stiffening progressively reduces the valve opening area. A normal aortic valve area measures approximately three to four square centimetres. Severe Aortic Stenosis is defined by a valve area below one square centimetre, representing more than a 75 percent reduction in functional opening size.
The Heart’s Response to Obstruction
Facing this obstruction, the left ventricle generates enormous pressure to force blood through the narrowed valve. Over time, this sustained pressure overload causes the ventricular wall to thicken in a process called concentric hypertrophy. While initially compensatory, this thickening ultimately makes the ventricle stiffer, impairs its filling, and increases the risk of dangerous arrhythmias and heart failure.
This progressive deterioration explains why Aortic Stenosis, once considered a gradual benign condition, demands careful monitoring and timely intervention before irreversible ventricular damage develops.
Why Aortic Stenosis Is Increasingly Common in Older Adults
The rising prevalence of Aortic Stenosis directly reflects global demographic trends. As populations age, more people reach the decades of life where degenerative valve calcification becomes increasingly common.
The Ageing Valve
The most common cause of Aortic Stenosis in developed countries is degenerative calcification, meaning calcium deposits accumulate progressively on the valve leaflets as part of the ageing process. This process resembles atherosclerosis, the same mechanism that causes coronary artery disease, and shares many of the same risk factors.
Studies estimate Aortic Stenosis affects approximately two to five percent of adults over 65 and up to eight to ten percent of those over 80. As life expectancy continues extending globally, epidemiologists project that Aortic Stenosis prevalence will more than double over the next two decades.
Shared Risk Factors With Coronary Artery Disease
Degenerative Aortic Stenosis shares risk factors with coronary artery disease. Hypertension, diabetes, high cholesterol, smoking, obesity, and male sex all accelerate valve calcification. People with these risk factors develop clinically significant Aortic Stenosis at earlier ages and with greater severity than those without them.
This overlap means cardiologists frequently encounter Aortic Stenosis alongside coronary artery disease, requiring integrated management strategies that address both conditions simultaneously.
Bicuspid Aortic Valve
A bicuspid aortic valve, a congenital abnormality present in approximately one to two percent of the population, causes early-onset Aortic Stenosis. Normally the aortic valve has three leaflets. When only two leaflets develop, the valve experiences abnormal mechanical stress throughout life, accelerating calcification by decades compared to the tricuspid valve.
People with bicuspid aortic valves typically develop significant Aortic Stenosis in their fifties and sixties rather than in their seventies and eighties. This condition also carries associated risks of aortic root enlargement requiring monitoring.
Causes of Aortic Stenosis
Understanding the distinct causes of Aortic Stenosis clarifies the different clinical presentations and guides surveillance strategies.
Degenerative Calcific Aortic Stenosis
Degenerative calcification is responsible for the majority of Aortic Stenosis cases in adults over 65. Calcium deposits accumulate on the valve cusps over decades, stiffening the leaflets and progressively reducing their mobility. The process begins as aortic valve sclerosis, mild thickening without obstruction, and advances to frank stenosis over years.
The rate of progression varies considerably between individuals. On average, the valve area decreases by approximately 0.1 square centimetres per year in established stenosis. However, progression can be substantially faster in some people, particularly those with heavy calcium burden.
Rheumatic Heart Disease
Rheumatic fever, triggered by untreated streptococcal throat infections, causes scarring and fusion of heart valve leaflets. Rheumatic Aortic Stenosis develops decades after the initial infection and frequently coexists with mitral valve disease. This cause predominantly affects people in low- and middle-income countries where rheumatic fever remains common.
Globally, rheumatic heart disease remains a leading cause of Aortic Stenosis in younger adults, contrasting with the degenerative cause dominant in higher-income countries.
Congenital Causes
Beyond bicuspid aortic valve, other congenital valve abnormalities including unicuspid valves occur rarely and cause severe early-onset Aortic Stenosis, sometimes requiring intervention in childhood or early adulthood.
Symptoms of Aortic Stenosis
Aortic Stenosis has a characteristic natural history. People remain asymptomatic, meaning without symptoms, for many years during the gradual valve narrowing process. Once symptoms appear, however, prognosis deteriorates dramatically without treatment.
The Classic Symptom Triad
Three cardinal symptoms define severe symptomatic Aortic Stenosis. Angina, meaning chest pain or pressure on exertion, develops as the thickened ventricle outstrips its blood supply. Syncope, meaning episodes of fainting or near-fainting, occurs when the narrowed valve prevents adequate blood flow to the brain during physical activity.
Heart failure symptoms including breathlessness, reduced exercise tolerance, and fluid retention develop as the ventricle progressively decompensates. The onset of any of these three symptoms signals a critical transition point in Aortic Stenosis natural history.
Survival Without Treatment After Symptoms Appear
Historical data demonstrates the grim prognosis once symptoms develop without valve intervention. Survival after angina onset averages approximately five years. Survival after syncope averages approximately three years. Survival after heart failure onset averages less than two years.
These statistics underscore why symptom onset triggers urgent cardiological evaluation and typically prompts early intervention planning rather than watchful waiting.
Asymptomatic Disease
During the asymptomatic phase, many people with severe Aortic Stenosis feel entirely well and lead normal lives. The only clinical finding may be a distinctive heart murmur detected incidentally during routine examination.
Distinguishing truly asymptomatic patients from those who have gradually reduced their activity to avoid exertional symptoms requires careful history-taking. Some people unconsciously limit activities that would provoke symptoms, masking the true severity of their functional impairment.
Exercise Testing in Aortic Stenosis
Supervised exercise testing helps identify genuinely asymptomatic severe Aortic Stenosis patients versus those with occult symptoms. Some patients demonstrate abnormal blood pressure responses, ST segment changes suggesting inadequate cardiac blood flow, or symptom development during exercise testing despite denying symptoms at rest.
These findings identify a higher-risk subgroup who may benefit from earlier intervention despite apparent clinical silence.
Diagnosing Aortic Stenosis
Accurate diagnosis and severity assessment guide the timing of intervention, which is the most critical management decision in Aortic Stenosis.
Auscultation and Heart Murmur
Aortic Stenosis produces a characteristic heart murmur audible with a stethoscope. Turbulent blood flow through the narrowed valve creates a harsh, crescendo-decrescendo systolic murmur, meaning one that peaks in intensity during mid-systole. This murmur radiates characteristically toward the carotid arteries in the neck.
The murmur’s loudness correlates imperfectly with severity. In very advanced disease with a failing ventricle generating little forward flow, the murmur may paradoxically soften, potentially misleading clinicians unfamiliar with this phenomenon.
Echocardiography
Echocardiography is the definitive investigation for Aortic Stenosis diagnosis and severity grading. Transthoracic echocardiography measures the valve area, the pressure gradient across the valve, and the aortic jet velocity, three parameters that together define Aortic Stenosis severity.
Severe Aortic Stenosis is defined by a mean pressure gradient exceeding 40 mmHg, a peak jet velocity above four metres per second, or a valve area below one square centimetre. Echocardiography simultaneously assesses left ventricular function, wall thickness, and diastolic parameters critical for intervention planning.
Doppler Echocardiography
Doppler technology within echocardiography measures blood flow velocity precisely. In severe Aortic Stenosis, blood accelerates dramatically through the narrowed valve opening, producing measurable velocity increases that allow accurate gradient calculation without invasive catheterisation.
Serial echocardiographic surveillance tracks disease progression over time, guiding the interval between assessments based on current severity.
CT Calcium Scoring
Computed tomography calcium scoring of the aortic valve directly quantifies calcium burden on the valve leaflets. High calcium scores correlate strongly with severe stenosis and predict more rapid progression. CT calcium scoring proves particularly valuable when echocardiographic severity assessment is discordant or inconclusive, resolving diagnostic uncertainty in challenging cases.
CT also provides detailed anatomical information about aortic root dimensions and peripheral vascular access routes essential for transcatheter valve procedure planning.
Cardiac Catheterisation
Invasive cardiac catheterisation is rarely needed for Aortic Stenosis severity assessment since echocardiography became highly accurate. However, coronary angiography, performed through catheterisation, remains essential before valve intervention to identify coexistent coronary artery disease requiring simultaneous treatment.
Treatment of Aortic Stenosis
No medication slows the progression of calcific Aortic Stenosis or reverses established valve disease. Once significant Aortic Stenosis develops, the only effective treatment is valve replacement or repair.
Medical Management of Asymptomatic Disease
During the asymptomatic surveillance phase, medical management focuses on treating risk factors and comorbidities rather than the valve itself. Hypertension, diabetes, and dyslipidaemia all require optimal management. Diuretics address fluid retention in patients with coexisting heart failure.
Importantly, medications are used cautiously in severe Aortic Stenosis. Vasodilators and excessive diuretic use can reduce cardiac filling pressure dangerously in patients whose fixed outlet obstruction limits the heart’s ability to maintain blood pressure.
Surgical Aortic Valve Replacement
Surgical aortic valve replacement (SAVR) has been the gold standard treatment for decades. Under general anaesthesia with cardiopulmonary bypass, surgeons remove the diseased valve and implant a prosthetic replacement, either a mechanical valve or a tissue bioprosthesis.
Mechanical valves last a lifetime but require lifelong anticoagulation with warfarin to prevent thrombosis. Tissue valves avoid the need for anticoagulation but typically degenerate and require re-intervention after 10 to 20 years. The choice between valve types depends on age, lifestyle, bleeding risk, and patient preference.
Transcatheter Aortic Valve Replacement
Transcatheter Aortic Valve Replacement, universally called TAVR or TAVI, has revolutionised Aortic Stenosis treatment and represents one of cardiology’s most transformative advances of the past two decades. A collapsed prosthetic valve is delivered through a catheter, typically via the femoral artery in the groin, and deployed directly within the diseased native valve without open-heart surgery.
TAVR initially targeted patients too high-risk or frail for surgery. Successive clinical trials demonstrated non-inferiority or superiority of TAVR compared to surgical replacement across all surgical risk categories. Current guidelines now support TAVR as an appropriate option for most patients with severe symptomatic Aortic Stenosis, regardless of surgical risk.
Choosing Between TAVR and SAVR
The choice between TAVR and surgical replacement involves multidisciplinary heart team discussion considering age, anatomy, surgical risk, valve anatomy, coexistent coronary disease, and patient preference. For older adults above 75 and those with significant comorbidities, TAVR is typically preferred. For younger patients, particularly below 65, surgical replacement may offer better long-term valve durability.
This individualised approach, incorporating patient values and anatomical suitability, defines contemporary Aortic Stenosis care at experienced valve centres.
Balloon Valvuloplasty
Balloon valvuloplasty involves inflating a balloon catheter within the narrowed aortic valve to temporarily increase its opening. This procedure provides short-term symptomatic relief but does not address valve calcification durably, with restenosis occurring within months in most cases.
Valvuloplasty finds use as a bridge to definitive valve replacement in haemodynamically unstable patients or as a palliative measure in those not suitable for replacement. It does not represent a definitive treatment strategy in isolation.
Recovery and Life After Valve Replacement
Life after successful aortic valve replacement transforms for most people with symptomatic Aortic Stenosis, offering dramatic symptom improvement and extended survival.
Recovery From TAVR
TAVR recovery is remarkably rapid compared to open-heart surgery. Most patients mobilise within 24 hours and leave hospital within two to three days. Full functional recovery typically occurs within two to four weeks, allowing return to normal activities far sooner than after surgical replacement.
Temporary cardiac pacing requirements, vascular access site complications, and paravalvular leak, meaning small leaks around the prosthetic valve, are specific TAVR complications that cardiac teams monitor carefully during and after the procedure.
Recovery From Surgical Valve Replacement
Surgical replacement requires six to twelve weeks of full recovery. Sternal healing after the chest incision takes several months. Cardiac rehabilitation programmes are strongly recommended after surgical replacement, providing supervised exercise training, education, and psychological support that optimise long-term outcomes.
Long-Term Valve Surveillance
All prosthetic valves require long-term surveillance with annual clinical review and periodic echocardiography. Tissue valves show progressive degeneration over time, with clinical signs of re-stenosis or regurgitation emerging years after implantation. Mechanical valves require consistently therapeutic anticoagulation monitoring to prevent potentially catastrophic valve thrombosis.
People with prosthetic valves also require antibiotic prophylaxis before certain dental and surgical procedures to prevent infective endocarditis, a serious infection of the valve.
Special Considerations in Aortic Stenosis Management
Several specific circumstances require tailored management approaches in Aortic Stenosis care.
Low-Flow, Low-Gradient Aortic Stenosis
A particularly challenging subgroup involves patients with apparently severe Aortic Stenosis but low pressure gradients across the valve, often because the weakened ventricle generates insufficient flow to produce high gradients. Low-dose dobutamine stress echocardiography differentiates true severe stenosis from pseudo-severe stenosis caused by a weakened ventricle that opens the valve poorly.
Correctly identifying true severe low-flow Aortic Stenosis in this group ensures these patients receive the intervention that can genuinely improve their outcomes and survival.
Aortic Stenosis in Frail Older Adults
Frailty assessment has become integral to Aortic Stenosis management in older adults. Very frail patients face higher procedural risks and may derive limited benefit from valve replacement if frailty and comorbidity dominate their prognosis. Formal frailty scoring using validated tools guides shared decision-making conversations about intervention versus palliative management.
Advance care planning discussions should accompany these conversations, ensuring each person’s values and goals genuinely inform every treatment decision.
Frequently Asked Questions
What is Aortic Stenosis?
Aortic Stenosis is a progressive narrowing of the aortic valve, the heart’s main outlet valve, due to calcium accumulation, congenital abnormality, or rheumatic scarring. This narrowing obstructs blood flow from the left ventricle to the aorta, forcing the heart to work much harder. Over time, this extra strain causes the ventricular wall to thicken and eventually weakens it, leading to heart failure without treatment.
What are the warning signs of Aortic Stenosis?
The three classic warning symptoms are chest pain or pressure on exertion, unexplained fainting or near-fainting especially during activity, and breathlessness reflecting developing heart failure. Many people also experience progressive fatigue and reduced exercise tolerance. Symptom onset marks a critical deterioration point in Aortic Stenosis, making immediate cardiological assessment essential once any of these symptoms develop.
Can Aortic Stenosis be treated without surgery?
No medication reverses or halts calcific Aortic Stenosis progression. Once severe symptomatic Aortic Stenosis develops, valve replacement is the only effective treatment. Transcatheter Aortic Valve Replacement (TAVR) now offers a minimally invasive option avoiding open-heart surgery, making valve replacement accessible to very elderly or frail patients who previously had no good treatment options.
How serious is Aortic Stenosis?
Once symptoms develop, Aortic Stenosis becomes a serious and life-limiting condition without treatment. Historical survival data shows dramatically shortened life expectancy after angina, syncope, or heart failure onset without valve replacement. With timely intervention, most people experience dramatic symptom improvement and survival prolongation comparable to age-matched populations without valve disease.
What is TAVR and who is it suitable for?
Transcatheter Aortic Valve Replacement is a minimally invasive procedure delivering a prosthetic valve through a catheter, typically via the femoral artery, without open-heart surgery. Originally developed for high-surgical-risk patients, TAVR now has evidence supporting its use across all risk categories. It is particularly suited to older adults, frail patients, and those with significant comorbidities who benefit from avoiding the physiological stress of open-heart surgery.
How long do replacement aortic valves last?
Mechanical valve replacements last indefinitely but require lifelong anticoagulation. Tissue bioprostheses last approximately 10 to 20 years before progressive deterioration requires re-intervention. TAVR tissue valves appear to have durability similar to surgical tissue valves based on medium-term follow-up data, though very long-term data continues to accumulate. Valve choice depends on age, lifestyle, anticoagulation suitability, and individual preference after discussion with a specialist.
Disclaimer:
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis, treatment, or medical guidance related to any health condition.
References:
- Connective tissue is exactly what it sounds like—tissue that connects, supports, and holds together all the organs and structures in your body.
- Moyamoya disease is a rare progressive cerebrovascular disorder characterized by progressive stenosis of distal internal carotid arteries and abnormal collateral vessel development.
- Despite the reassurances from Valve, the company advised Steam users to remain vigilant.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.