
Overactive Bladder: Causes, Treatments, and What’s Going On
Imagine being in a meeting, on a bus, or in the middle of a meal — and suddenly feeling an overwhelming, impossible-to-ignore urge to urinate. Not a gentle reminder. A sudden, urgent command that demands immediate action. For millions of people worldwide, this is not an occasional inconvenience. It is a daily reality.
Overactive bladder — commonly called OAB — is a condition in which the bladder contracts too often and too urgently, sending false signals to the brain that it needs to be emptied even when it is not full. It causes a sudden, compelling urge to urinate that can be very difficult to control. As a result, people with OAB often urinate far more frequently than normal and may leak urine before reaching the bathroom.
Overactive bladder causes treatments OAB is a topic that matters enormously to quality of life. OAB affects an estimated 33 million people in the United States alone — and hundreds of millions more worldwide. Furthermore, it affects people of all ages, sexes, and backgrounds, though it becomes more common with age. However, despite being very common, OAB remains widely underreported because many people feel embarrassed to discuss it. Consequently, millions of people live with manageable symptoms unnecessarily when effective treatments are readily available.
Quick Answer
Overactive bladder — OAB — is a condition in which the bladder muscle contracts too frequently, causing sudden urinary urgency, frequent urination, and sometimes urinary leakage. It results from abnormal nerve signals between the bladder and brain. Treatment includes bladder training, pelvic floor exercises, medications, and — when needed — minimally invasive procedures.
What Is Overactive Bladder?
How the Bladder Normally Works
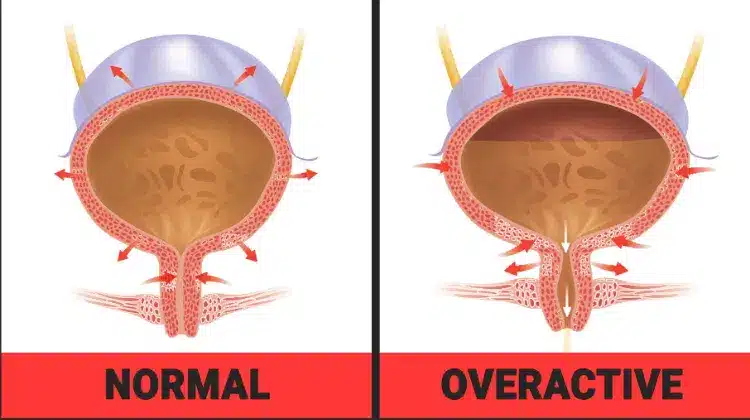
The bladder is a hollow, muscular organ that stores urine produced by the kidneys. It has two jobs — storing urine comfortably while it fills and releasing it at an appropriate time. The bladder wall contains a layer of smooth muscle called the detrusor muscle. This muscle remains relaxed while the bladder fills and only contracts when a person chooses to urinate.
A complex set of nerve signals coordinates this process. As the bladder fills, stretch receptors in the bladder wall send signals to the brain indicating fullness. The brain then sends back signals to either maintain relaxation — suppressing the urge — or trigger contraction when the timing is right. In healthy bladder function, a person typically urinates six to eight times per day and can comfortably hold urine for two to four hours between visits.
What Goes Wrong in OAB
In overactive bladder, the detrusor muscle contracts involuntarily — squeezing even when the bladder is only partially full. These unexpected contractions send sudden, intense urge signals to the brain. Consequently, the brain receives an urgent message to urinate even though the bladder has not filled to its normal capacity.
Doctors call this abnormal pattern detrusor overactivity. It is not a problem with the bladder structure itself — the bladder looks normal on imaging. Instead, the problem lies in the nerve signalling pathways between the bladder, spinal cord, and brain. As a result, the communication system that normally keeps urination under voluntary control breaks down. For broader context on how bladder conditions relate to kidney and urinary tract health, see our article on chronic kidney disease — stages, symptoms, and how to slow the decline.
Causes of Overactive Bladder
Neurological and Age-Related Causes
Overactive bladder causes treatments OAB begins with understanding why the bladder becomes overactive in the first place. Several factors contribute, and in many cases more than one factor operates simultaneously.
Age is the most important risk factor. As people age, the nerve pathways controlling the bladder become less efficient. The central nervous system — the brain and spinal cord — gradually loses some of its ability to suppress unwanted bladder contractions. Consequently, bladder urgency and frequency increase with age even in people without specific underlying conditions.
Neurological conditions are a major cause of OAB in younger people. Multiple sclerosis, Parkinson’s disease, stroke, and spinal cord injuries all disrupt the nerve signals controlling the bladder and cause detrusor overactivity. In addition, diabetic neuropathy — nerve damage caused by long-term diabetes — affects the bladder nerves and produces OAB symptoms in a significant proportion of people with diabetes.
Bladder and Lifestyle Triggers
Bladder outlet obstruction — where the flow of urine out of the bladder is partially blocked — causes the detrusor muscle to work harder than normal. Over time, this increased workload thickens the muscle and makes it more prone to involuntary contractions. In people with penises, enlarged prostate — called benign prostatic hyperplasia — is one of the most common causes of outlet obstruction leading to OAB. For more on how prostate enlargement affects urinary function, see our article on benign prostatic hyperplasia — the enlarged prostate explained.
Urinary tract infections irritate the bladder lining and trigger urgency that closely mimics OAB. Bladder stones, bladder tumours, and interstitial cystitis — a chronic painful bladder condition — can all produce similar symptoms. Furthermore, certain dietary triggers — including caffeine, alcohol, carbonated drinks, and highly acidic foods — irritate the bladder directly and worsen OAB symptoms in susceptible individuals. For context on chronic bladder pain that can overlap with OAB symptoms, see our article on interstitial cystitis — the chronic condition behind UTI symptoms.
Hormonal and Pelvic Factors
Hormonal changes play a significant role in OAB — particularly in people who have gone through menopause. Falling oestrogen levels after menopause thin the tissues of the bladder and urethra, making them more sensitive and reactive. This contributes to the higher prevalence of OAB in postmenopausal women.
Pelvic floor weakness — reduced strength and coordination in the muscles that support the bladder and urethra — contributes to OAB by reducing the ability to suppress urgency and delay urination. Pregnancy and childbirth, obesity, and previous pelvic surgery all weaken pelvic floor muscles and consequently increase OAB risk. Moreover, chronic constipation places pressure on the bladder from the adjacent rectum and worsens urgency and frequency.
Symptoms of Overactive Bladder
The Core Symptom Pattern
Overactive bladder causes treatments OAB produces a distinctive and recognisable symptom pattern. Urinary urgency is the defining symptom. It is a sudden, strong, and very difficult-to-defer desire to urinate. Unlike the gradual build of a normal full bladder, urgency in OAB arrives abruptly and intensely. Furthermore, it often strikes in response to triggers — running water, cold air, putting a key in a door, or arriving home — a phenomenon sometimes called latchkey urgency.
Urinary frequency — needing to urinate eight or more times in a 24-hour period — accompanies urgency in most people with OAB. Nocturia — waking one or more times during the night to urinate — is particularly disruptive and significantly impairs sleep quality and daytime functioning. Moreover, it increases the risk of falls in older adults who rush to the bathroom in the dark.
Urge Incontinence
Urge incontinence — the involuntary leakage of urine that occurs when urgency cannot be suppressed in time — affects roughly one third of people with OAB. It represents the most socially and psychologically disruptive aspect of the condition. Many people reduce social activities, avoid travelling, stop exercising, and limit their fluid intake in an attempt to manage leakage. However, excessive fluid restriction paradoxically concentrates the urine and irritates the bladder further — worsening rather than improving symptoms.
It is important to distinguish OAB from stress incontinence — leakage that occurs during physical effort such as coughing, sneezing, or exercise. Stress incontinence results from weakness of the urethral sphincter rather than bladder overactivity. Some people experience both types simultaneously — a pattern called mixed incontinence. Consequently, accurately identifying the type of incontinence present guides the correct treatment approach.
How Doctors Diagnose Overactive Bladder
Clinical Assessment
Diagnosing overactive bladder causes treatments OAB suitability begins with a thorough clinical history. Doctors ask about the frequency and severity of urgency, the number of daily and nighttime voids, the presence and circumstances of leakage, fluid intake habits, and the impact of symptoms on daily life. The Overactive Bladder Symptom Score — OABSS — and the International Consultation on Incontinence Questionnaire — ICIQ — provide validated tools for quantifying symptom severity.
A bladder diary — a three-day record of fluid intake, voiding times, and leakage episodes — provides objective data that guides both diagnosis and treatment monitoring. Furthermore, it helps identify dietary and behavioural triggers that a person may not have previously connected to their symptoms.
Tests to Rule Out Other Conditions
Urine dipstick and culture exclude urinary tract infection. Blood tests assess kidney function and blood sugar — screening for diabetes-related bladder nerve damage. For context on how kidney conditions can present alongside bladder symptoms, see our article on nephrotic syndrome — what protein in the urine actually tells you.
Post-void residual measurement — using ultrasound to check how much urine remains in the bladder after urinating — excludes incomplete emptying caused by outlet obstruction. Urodynamic testing — measuring pressure and flow during bladder filling and emptying — identifies detrusor overactivity objectively and distinguishes OAB from other causes of urgency and incontinence. Cystoscopy — examining the inside of the bladder with a thin camera — excludes bladder tumour, stones, and interstitial cystitis when symptoms are atypical or do not respond as expected to standard OAB treatment.
Treatment of Overactive Bladder
Behavioural Therapies
Treating overactive bladder causes treatments OAB always starts with behavioural strategies. These are the safest, most durable, and most cost-effective treatments available — and they work for the majority of people with mild to moderate OAB.
Bladder training is the most important behavioural intervention. It involves deliberately extending the time between urinations — starting with small increments of five to ten minutes — to gradually retrain the bladder to tolerate increasing volumes before triggering urgency. Over six to twelve weeks, most people significantly increase their bladder capacity and reduce urgency frequency. Furthermore, urgency suppression techniques — including deep slow breathing, mental distraction, and pelvic floor squeezing — help interrupt the urgency signal and allow the urge to pass without rushing to the bathroom.
Pelvic floor muscle training — also called Kegel exercises — strengthens the muscles that support the urethra and bladder and improves the ability to actively suppress urgency. A specialist pelvic floor physiotherapist provides the most effective guidance, including biofeedback — a technique that uses sensors to show muscle activity in real time. Moreover, fluid and dietary management — reducing caffeine, alcohol, and bladder-irritating foods while maintaining adequate hydration — reduces the chemical irritation driving detrusor overactivity.
Medications for OAB
When behavioural therapies alone provide insufficient relief, medication is the next step. Two main classes of medications treat OAB effectively.
Antimuscarinics — also called anticholinergics — block the nerve receptors on the detrusor muscle that trigger involuntary contractions. Commonly used antimuscarinics include oxybutynin, solifenacin, tolterodine, and darifenacin. They reduce urgency frequency and improve continence in most patients. However, they commonly cause dry mouth, constipation, blurred vision, and — particularly in older adults — cognitive side effects including confusion and memory problems. Consequently, they require careful use in people over 65.
Mirabegron is a newer class of OAB medication called a beta-3 adrenoceptor agonist. Instead of blocking muscle contraction signals, it relaxes the detrusor muscle directly during bladder filling. It is as effective as antimuscarinics but produces a significantly better side effect profile — without dry mouth or cognitive effects. Furthermore, mirabegron is now recommended as a first-line medication option for OAB in many international guidelines, particularly for older adults and those intolerant of antimuscarinics. Combining mirabegron with a low-dose antimuscarinic produces greater benefit than either alone in patients with persistent symptoms.
Advanced Treatments
For patients who do not respond adequately to behavioural therapies and medications, advanced treatment options are available. Onabotulinumtoxin A — commonly known as Botox — injected directly into the detrusor muscle using a cystoscope significantly reduces involuntary bladder contractions. It provides relief for six to twelve months before repeat injection is required. Moreover, it is highly effective even in patients who have failed multiple medications. The main side effect is urinary retention — incomplete bladder emptying — which occurs in a minority of patients and requires temporary self-catheterisation.
Sacral neuromodulation — also called bladder pacemaker therapy — involves implanting a small device near the sacral nerve in the lower back. This device sends mild electrical impulses that modulate the abnormal nerve signals driving bladder overactivity. Consequently, it produces durable long-term improvement in urgency, frequency, and urge incontinence in carefully selected patients. Percutaneous tibial nerve stimulation — PTNS — delivers similar nerve modulation effects through a less invasive approach, using a fine needle near the ankle to stimulate a nerve pathway that connects to the bladder. Furthermore, PTNS requires weekly outpatient sessions over twelve weeks before benefit is fully established.
For broader context on how kidney stones can cause urinary symptoms that mimic or coexist with OAB, see our article on kidney stones — types, causes, prevention, and pain management.
Living Well With Overactive Bladder
Managing Daily Life and Emotional Wellbeing
Overactive bladder significantly affects emotional wellbeing, social participation, and relationship quality. Anxiety about leakage restricts travel, exercise, work, and social activities. Many people with OAB feel embarrassed, isolated, and reluctant to discuss their symptoms — even with a doctor. As a result, treatment is often delayed by years.
Normalising OAB as a common medical condition — not a personal failing or an inevitable consequence of ageing — is an essential first step. Furthermore, involving a continence nurse specialist or pelvic health physiotherapist provides tailored guidance that significantly improves outcomes beyond what medication alone can achieve. Patient support groups and continence advisory services offer practical tools, peer support, and emotional validation that many people with OAB find transformative.
Monitoring and Long-Term Management
OAB is a long-term condition for many people, though symptoms can improve significantly with the right treatment combination. Regular review with a healthcare provider allows adjustment of the management plan as symptoms evolve. Moreover, keeping a bladder diary at intervals helps track progress and identify new triggers or symptom changes that warrant clinical attention.
Any person with OAB who develops new blood in the urine, significant pain, or a sudden change in symptoms needs prompt medical review to exclude other conditions including bladder cancer, kidney stones, or kidney damage. For context on how kidney health is assessed in people with urological conditions, see our article on chronic kidney disease — stages, symptoms, and how to slow the decline.
When to Seek Medical Help
See a doctor promptly if you experience urinary urgency that significantly affects your daily life, urge incontinence, nocturia waking you more than twice per night, or urinary frequency greater than eight times per day. These symptoms are not a normal part of ageing and they deserve proper medical evaluation.
Furthermore, seek urgent medical attention if you develop blood in the urine alongside OAB symptoms, sudden inability to urinate, fever with urinary symptoms, or new neurological symptoms such as leg weakness or numbness. Consequently, early assessment ensures that treatable underlying conditions are identified promptly and that effective management begins without unnecessary delay.
Frequently Asked Questions
1. Is overactive bladder the same as urinary incontinence?
Not exactly. Overactive bladder is a condition defined by urgency — with or without leakage. Urinary incontinence is the broader term for any involuntary urine leakage. OAB causes urge incontinence — leakage driven by a sudden, uncontrollable urge. However, other types of incontinence — particularly stress incontinence caused by physical exertion — occur without OAB. Consequently, accurately identifying which type of incontinence is present determines which treatment approach will be most effective.
2. Can overactive bladder be cured permanently?
In some people, yes — particularly when OAB results from a treatable underlying cause such as a urinary tract infection, bladder stone, or reversible hormonal change. However, for many people, OAB is a long-term condition that requires ongoing management. Moreover, behavioural therapies and medications can achieve very significant and sustained symptom improvement even when complete cure is not possible. Consequently, the realistic goal for most patients is meaningful symptom control that restores normal daily activities and quality of life.
3. Does drinking less water help with overactive bladder?
Restricting fluid intake is a common self-management strategy but it often makes symptoms worse rather than better. When a person drinks too little, urine becomes highly concentrated. Concentrated urine irritates the bladder lining directly and triggers more urgent and frequent urges. Furthermore, concentrated urine increases the risk of urinary tract infections and kidney stones. Consequently, maintaining adequate fluid intake — spread evenly throughout the day and reduced in the evening — is more effective than significant fluid restriction.
4. Is overactive bladder more common in women than men?
OAB affects both sexes but the pattern differs. In women, OAB is closely linked to pelvic floor changes, menopause, pregnancy, and childbirth. In men, it is frequently associated with prostate enlargement causing bladder outlet obstruction. Furthermore, urgency incontinence — leakage with urgency — is significantly more common in women than in men. Consequently, treatment approaches are often tailored to the sex-specific contributing factors in each individual. For more on how prostate enlargement contributes to OAB symptoms in men, see our article on benign prostatic hyperplasia — the enlarged prostate explained.
5. Can children develop overactive bladder?
Yes. Overactive bladder is relatively common in children and is a leading cause of daytime wetting and bedwetting beyond the expected age of toilet training. In children, the condition often reflects delayed maturation of the bladder control pathways in the nervous system. Furthermore, stress, constipation, urinary tract infections, and poor voiding habits can all contribute to OAB symptoms in children. Consequently, a child with persistent urinary urgency, frequency, or daytime wetting beyond age five deserves a proper medical evaluation rather than simple reassurance that they will grow out of it.
References
- Hyperthyroidism refers to increased thyroid hormone synthesis and secretion, most commonly from Graves’ disease or toxic nodular goitre.
- The bladder is a hollow, muscular organ in the pelvis that stores urine produced by the kidneys
- During the ongoing COVID-19 pandemic, there are many social, cultural changes are observed around the globe.
- Normal Pressure Hydrocephalus, commonly called NPH
- Normal pressure hydrocephalus is a neurological disorder where impaired CSF absorption leads to ventricular enlargement and progressive neurological dysfunction despite normal intracranial pressure.
Disclaimer
This article adapts publicly available information from WHO’s Noncommunicable Diseases page. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform and not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.