
Infective Endocarditis: When Bacteria Attack the Heart Valves
The heart valves open and close more than 100,000 times every day. This relentless mechanical activity makes them vulnerable in ways that most people never consider. When bacteria enter the bloodstream and attach to these valves, they can trigger a dangerous infection called infective endocarditis.
This condition is a medical emergency. Without prompt diagnosis and treatment, infective endocarditis can destroy heart valves, spread infection to other organs, and prove fatal. Understanding this disease helps patients recognise warning signs before irreversible damage occurs.
What Is Infective Endocarditis?
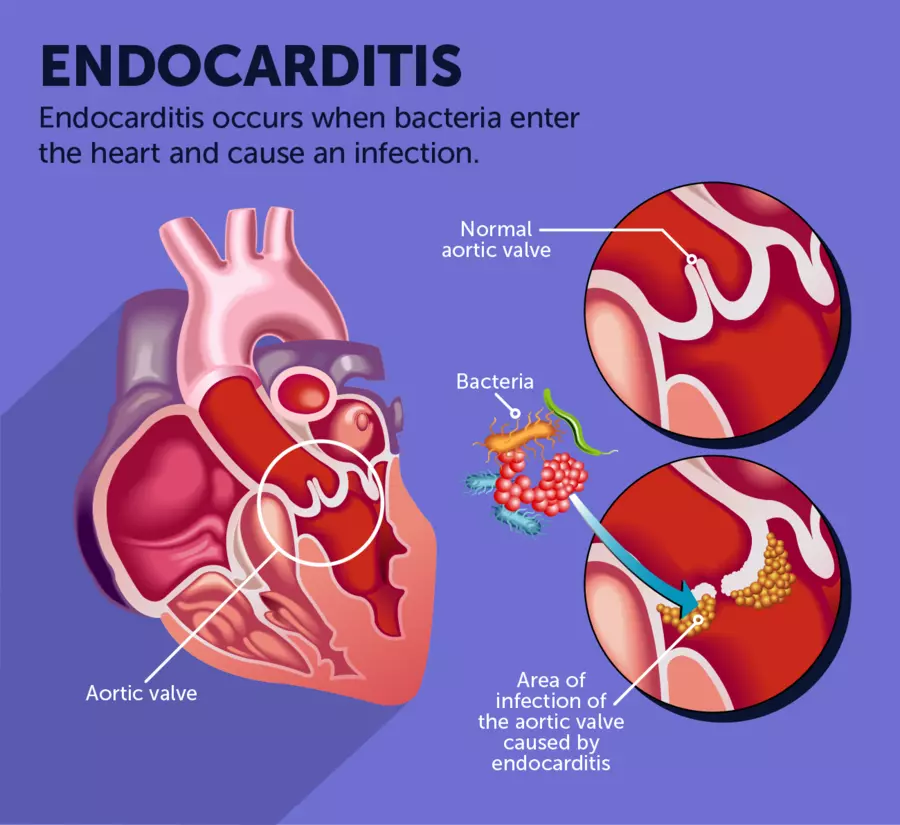
Infective endocarditis (IE) is an infection of the inner lining of the heart chambers and valves, known as the endocardium. Bacteria, and less commonly fungi, attach to the valve surface and form clumps of infected tissue called vegetations. These vegetations are clusters of microorganisms, blood cells, and fibrin — the protein that forms blood clots.
How the Infection Takes Hold
Normally, bacteria that enter the bloodstream are quickly eliminated by the immune system. However, damaged or abnormal heart valves create rough or irregular surfaces where bacteria can more easily anchor and multiply. Once established, the infection grows rapidly and becomes increasingly difficult to eradicate without aggressive treatment.
Vegetations can grow large enough to impair valve function. They can also break off and travel through the bloodstream, blocking arteries in the brain, kidneys, lungs, or limbs. These travelling clots, called emboli, cause strokes and organ damage that can be permanent.
Types of Infective Endocarditis
Doctors classify infective endocarditis in several ways based on the speed of onset, the valve affected, and whether a prosthetic (artificial) valve is involved.
Acute vs Subacute Endocarditis
Acute infective endocarditis develops rapidly, often over days to weeks. It is typically caused by highly aggressive bacteria such as Staphylococcus aureus, which can infect even normal, healthy valves. This form progresses quickly and demands immediate hospitalisation and treatment.
Subacute infective endocarditis develops more slowly, unfolding over weeks to months. It is commonly caused by less aggressive organisms such as Streptococcus viridans, which tend to infect previously damaged or abnormal valves. Symptoms are often subtle at first, which unfortunately delays diagnosis.
Native vs Prosthetic Valve Endocarditis
Native valve endocarditis affects the heart’s own natural valves. Prosthetic valve endocarditis occurs in people who have received artificial heart valves through surgery or transcatheter procedures. Prosthetic valves carry a lifelong risk of infection, as bacteria can colonise the artificial material used in construction.
Right-Sided vs Left-Sided Endocarditis
Left-sided endocarditis, affecting the mitral and aortic valves, is the most common form. Right-sided endocarditis, affecting the tricuspid and pulmonary valves, occurs predominantly in people who inject drugs intravenously, as bacteria enter directly through contaminated needles.
What Causes Infective Endocarditis?
Infective endocarditis develops when bacteria or fungi enter the bloodstream in a process called bacteraemia. This can occur through numerous everyday events, medical procedures, and certain health conditions.
Common Bacterial Causes
Staphylococcus aureus is now the leading cause of infective endocarditis globally. It is a highly virulent bacterium that spreads aggressively and can infect structurally normal valves. Healthcare-associated infections, intravenous drug use, and skin wounds are common sources of S. aureus bacteraemia.
Streptococcal species, including Streptococcus viridans from the mouth, cause a significant proportion of cases. Oral bacteria enter the bloodstream during dental procedures, tooth brushing, or even chewing. People with pre-existing valve disease are particularly vulnerable to streptococcal endocarditis.
Other Microbial Causes
The HACEK group of bacteria — Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, and Kingella — are slow-growing organisms found in the mouth and throat that occasionally cause endocarditis. Enterococcal species, typically originating from the gut or urinary tract, are another important cause, especially in older adults following urological procedures.
Fungal endocarditis is rare but serious. Candida and Aspergillus species are responsible for most fungal cases, occurring predominantly in immunocompromised individuals and those with prosthetic valves.
How Bacteria Enter the Bloodstream
Bacteria reach the bloodstream through dental procedures, surgical interventions, skin infections, intravenous catheter use, and body piercing or tattooing performed with non-sterile equipment. Even routine activities such as vigorous tooth brushing can introduce small numbers of oral bacteria into the circulation. For most people, this poses no risk, but those with vulnerable hearts face a genuine threat.
Who Is at Risk?
Not everyone who develops bacteraemia will develop infective endocarditis. Certain underlying conditions significantly raise individual risk.
Structural Heart Conditions
People with congenital heart defects — heart abnormalities present from birth — carry a higher lifetime risk of infective endocarditis. Conditions such as bicuspid aortic valve, ventricular septal defect, and tetralogy of Fallot all create abnormal flow patterns that increase bacterial attachment risk.
Acquired valve disease, including rheumatic heart disease, mitral valve prolapse with valve regurgitation, and degenerative aortic stenosis, also elevates risk considerably. Rheumatic heart disease, caused by repeated streptococcal infections, remains a major risk factor in low- and middle-income countries.
Prosthetic Valves and Cardiac Devices
People with prosthetic heart valves face the highest risk of infective endocarditis. Artificial valve surfaces are particularly susceptible to bacterial colonisation. Similarly, implanted cardiac devices such as pacemakers and implantable cardioverter-defibrillators (ICDs) can serve as sites of infection.
Other Risk Factors
Intravenous drug use is a major and growing risk factor, primarily causing right-sided endocarditis. Haemodialysis patients, who require repeated vascular access, carry significantly elevated risk. Immunocompromised individuals, including those receiving chemotherapy or immunosuppressive medications, are also at higher risk of both bacteraemia and endocarditis.
Recognising the Symptoms
Infective endocarditis presents with a wide range of symptoms, making early recognition challenging. Symptoms vary depending on the causative organism, the valve involved, and whether embolic complications have occurred.
Fever and Constitutional Symptoms
Persistent fever is the most common symptom of infective endocarditis, occurring in the vast majority of patients. Accompanying fever, patients typically experience chills, night sweats, and profound fatigue. These constitutional symptoms often resemble a flu-like illness, which can mislead both patients and clinicians during the early stages.
Unexplained weight loss and loss of appetite are additional hallmarks. These features reflect the body’s systemic inflammatory response to ongoing infection. Any persistent unexplained fever in a person with known cardiac risk factors should prompt urgent investigation.
Cardiac Symptoms
A new or changing heart murmur is a cardinal sign of infective endocarditis. Murmurs arise when vegetations or valve damage disrupt the normal smooth flow of blood through the heart. Doctors use a stethoscope to detect these abnormal sounds during physical examination.
Breathlessness, reduced exercise tolerance, and signs of heart failure may develop as valve destruction progresses. Rapid deterioration in cardiac function represents a surgical emergency and demands immediate intervention.
Embolic and Vascular Signs
Embolic complications affect up to 50% of patients with infective endocarditis. Stroke, transient ischaemic attack (TIA), and sudden limb pain or loss of function can all result from vegetations breaking free and blocking arteries.
Certain classic physical signs — now less commonly seen due to earlier diagnosis — include Janeway lesions (painless red spots on the palms and soles), Osler’s nodes (painful nodules on fingers and toes), Roth spots (retinal haemorrhages seen during eye examination), and splinter haemorrhages under the fingernails. These findings, when present, are highly suggestive of infective endocarditis.
How Doctors Diagnose Infective Endocarditis
Diagnosing infective endocarditis requires a combination of clinical assessment, blood cultures, and cardiac imaging. The modified Duke criteria provide a structured framework that clinicians use to classify cases as definite, possible, or rejected.
Blood Cultures
Blood cultures are the cornerstone of diagnosis. Collecting blood samples before starting antibiotics allows laboratories to identify the causative organism and test its sensitivity to various antibiotics. Typically, at least three sets of blood cultures are taken from different sites to maximise the chances of detecting bacteria.
Culture-negative endocarditis occurs in approximately 10–15% of cases, often due to prior antibiotic use or infection with difficult-to-culture organisms. In these cases, specialised serological tests and molecular techniques help identify the pathogen.
Echocardiography
Echocardiography — an ultrasound scan of the heart — is the primary imaging tool for diagnosing infective endocarditis. Transthoracic echocardiography (TTE), which uses an external probe on the chest wall, provides initial assessment. However, transoesophageal echocardiography (TOE), which passes a probe down the oesophagus to image the heart from behind, offers superior detail and sensitivity.
TOE can detect smaller vegetations and is particularly valuable for assessing prosthetic valves and identifying complications such as abscesses or perforations. Most patients with suspected infective endocarditis require both forms of echocardiography.
Additional Investigations
A full blood count typically shows elevated white blood cells, reflecting active infection. Raised inflammatory markers — C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) — confirm ongoing systemic inflammation. Urine analysis may reveal blood or protein, suggesting embolic involvement of the kidneys.
Advanced imaging including CT scanning and PET-CT are increasingly used to detect metastatic infection, embolic events, and complications outside the heart. These tools add significant diagnostic value in complex or culture-negative cases.
Treatment of Infective Endocarditis
Treating infective endocarditis requires prolonged intravenous antibiotic therapy and, in many cases, cardiac surgery. Management is best delivered by a specialist multidisciplinary endocarditis team.
Antibiotic Therapy
High-dose intravenous antibiotics form the cornerstone of treatment. The choice of antibiotic depends on the causative organism and its antibiotic sensitivity profile. Treatment typically lasts between four and six weeks to ensure complete eradication of the infection.
Penicillin-based regimens remain effective for many streptococcal infections. Staphylococcal infections often require combinations including flucloxacillin, vancomycin (for resistant strains), and gentamicin. Antibiotic regimens are carefully tailored to culture and sensitivity results to maximise efficacy and minimise toxicity.
When Surgery Becomes Necessary
Approximately 50% of patients with infective endocarditis require cardiac surgery during their hospitalisation. Surgery aims to remove infected tissue, repair or replace damaged valves, and drain any abscesses that have formed around the heart.
Indications for urgent surgery include severe valve dysfunction causing heart failure, persistent infection despite appropriate antibiotics, large vegetations with high embolic risk, and cardiac abscesses. Timely surgery significantly improves survival in selected high-risk patients.
Managing Complications
Stroke management requires close collaboration between cardiology, neurology, and cardiac surgery teams. Anticoagulation decisions in patients with embolic stroke and prosthetic valves are particularly complex and must be individualised. Renal impairment, a common complication of both the infection and antibiotic therapy, requires careful monitoring and dose adjustments.
Preventing Infective Endocarditis
Prevention focuses on identifying high-risk individuals and implementing targeted protective strategies.
Antibiotic Prophylaxis Before Dental Procedures
Current guidelines recommend antibiotic prophylaxis before certain invasive dental procedures for patients at highest risk. High-risk groups include those with prosthetic heart valves, previous episodes of infective endocarditis, specific congenital heart defects, and heart transplant recipients with valvular disease.
A single dose of amoxicillin given 30–60 minutes before the procedure significantly reduces bacteraemia from dental manipulation. For people with penicillin allergy, clindamycin or azithromycin may be used as alternatives. Prophylaxis recommendations vary slightly between international guidelines, so patients should discuss their specific needs with their cardiologist.
Maintaining Oral Hygiene
Good oral hygiene is a cornerstone of endocarditis prevention for all at-risk individuals. Regular tooth brushing, flossing, and routine dental check-ups reduce the bacterial load in the mouth. Preventing gum disease and dental decay significantly lowers the frequency of oral bacteraemia.
Avoiding Preventable Risk Factors
Avoiding intravenous drug use eliminates one of the most significant preventable risk factors for right-sided endocarditis. Safe injection practices, harm reduction programmes, and substance use treatment services all contribute to reducing endocarditis incidence in this population. Ensuring sterile technique during medical procedures and proper care of vascular access devices also reduces hospital-acquired infections.
Living With and Recovering From Infective Endocarditis
Recovery from infective endocarditis is a prolonged process that requires patience, monitoring, and ongoing specialist care.
Hospital and Post-Discharge Care
Most patients require four to six weeks of intravenous antibiotics, often starting in hospital before completing the course at home or in an outpatient setting. Regular blood tests monitor antibiotic levels, kidney function, and inflammatory markers throughout treatment. Repeat echocardiography assesses valve function and confirms vegetation resolution.
Long-Term Follow-Up
Following recovery, regular cardiac follow-up is essential. Valve function requires ongoing surveillance, as damage sustained during infection can progress over time and eventually require surgical intervention. Patients who have experienced infective endocarditis remain at higher risk of recurrence throughout their lives.
Emotional Recovery
A serious illness like infective endocarditis affects mental wellbeing profoundly. Many survivors experience anxiety, depression, and post-traumatic stress, particularly following stroke or emergency surgery. Access to psychological support, peer networks, and patient education resources assists meaningful long-term recovery.
Frequently Asked Questions
How does infective endocarditis differ from other heart infections?
Infective endocarditis specifically infects the endocardium — the inner lining of the heart chambers and valves — through bacterial or fungal colonisation. Other heart infections include myocarditis, which affects the heart muscle, and pericarditis, which affects the outer sac surrounding the heart. Endocarditis is unique in its formation of vegetations on heart valves and its high risk of embolic complications.
Can infective endocarditis be cured completely?
Yes, many patients achieve complete cure with appropriate antibiotic therapy and, where necessary, surgery. However, permanent valve damage from the infection may require long-term monitoring or future surgical repair. Early diagnosis and prompt treatment significantly improve the chances of full recovery.
How long does treatment for infective endocarditis take?
Treatment typically requires four to six weeks of high-dose intravenous antibiotics. The precise duration depends on the causative organism, the valve affected, and whether complications have developed. Some patients complete part of their treatment in an outpatient or home-based intravenous therapy programme after initial stabilisation in hospital.
Is infective endocarditis contagious?
Infective endocarditis is not contagious between people. It develops when a person’s own bloodstream bacteria infect a vulnerable heart valve. The infection does not spread from person to person through contact, coughing, or other forms of transmission.
What happens if infective endocarditis goes untreated?
Untreated infective endocarditis is almost invariably fatal. Progressive valve destruction leads to severe heart failure, while embolising vegetations cause strokes, organ infarctions, and widespread sepsis. Even with modern treatment, infective endocarditis carries a significant in-hospital mortality rate of approximately 15–25%, underscoring the urgent need for early diagnosis.
Do people with heart murmurs need antibiotic prophylaxis?
Not all heart murmurs require antibiotic prophylaxis. Only patients at highest risk — including those with prosthetic valves, previous endocarditis, or specific complex congenital heart defects — are recommended prophylaxis before invasive dental procedures. A cardiologist can assess individual risk and provide clear, personalised guidance on the need for prophylaxis.
Conclusion
Infective endocarditis is a serious, potentially life-threatening infection that demands prompt recognition and expert treatment. Bacteria attacking the heart valves may seem like an improbable scenario, but for thousands of people each year, this is a devastating reality. Early awareness, timely medical care, and targeted prevention strategies make a genuine difference to outcomes.
If you have known heart disease, a prosthetic valve, or other cardiac risk factors, speak to your doctor about your personal risk. Protecting your heart starts with understanding the threats it faces. In the case of infective endocarditis, knowledge and vigilance can truly save lives.
References
- The aortic valve sits between the left ventricle and the aorta, the body’s largest artery.
- Wernicke-Korsakoff syndrome represents a severe neurological disorder resulting from thiamine, vitamin B1, deficiency affecting the brain.
- Despite the reassurances from Valve, the company advised Steam users to remain vigilant.
Disclaimer:
This article is for general informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personalised diagnosis, treatment, or health guidance.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.