
Raynaud’s Phenomenon: Why Fingers Turn White and Blue in the Cold
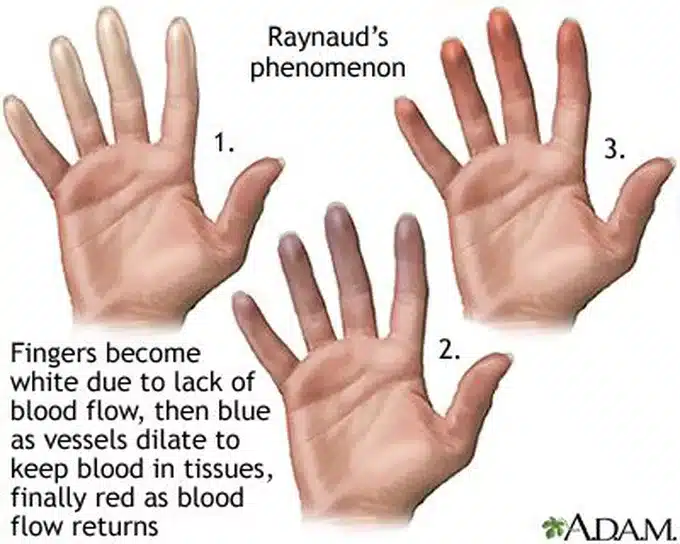
For most people, stepping into cold air means reaching for a coat. For those living with Raynaud’s phenomenon, the same experience triggers something far more dramatic — fingers that turn ghostly white, then blue, then painful red as blood flow cuts off and returns. This striking colour change is not simply about feeling cold. It reflects a genuine vascular disorder that affects millions of people worldwide.
Raynaud’s phenomenon is more common than many realise, yet it remains widely misunderstood. Some dismiss it as mere sensitivity to cold. In reality, it represents an exaggerated circulatory response that can significantly affect daily life — and in some cases, signals a serious underlying condition.
What Is Raynaud’s Phenomenon?
Raynaud’s phenomenon is a condition in which small blood vessels in the fingers and toes — and sometimes the ears, nose, lips, and nipples — react excessively to cold temperatures or emotional stress. This overreaction causes the vessels to spasm and narrow dramatically, cutting off blood supply to the affected areas.
The Vasospasm Explained
This sudden narrowing of blood vessels is called a vasospasm. During a vasospasm, blood flow to the extremities drops sharply and the skin loses its normal pink colour. The reduced circulation causes the characteristic colour changes that define a Raynaud’s attack.
Normal blood vessels respond to cold by constricting slightly to conserve core body heat. In Raynaud’s phenomenon, this response becomes massively exaggerated. Even mild temperature changes — such as reaching into a refrigerator or entering an air-conditioned room — can trigger a full attack in susceptible individuals.
The Three Colour Changes of a Raynaud’s Attack
The colour sequence during a Raynaud’s attack follows a recognisable three-phase pattern that reflects the changing state of blood flow through the affected digits.
White: The Blanching Phase
The first phase involves blanching — the fingers or toes turn white as vasospasm cuts off arterial blood flow almost entirely. The affected areas feel cold, numb, and may tingle uncomfortably. This phase can be startling to witness, as the colour change is sudden and striking.
Blue: The Cyanotic Phase
As blood remaining in the local tissues loses its oxygen, the skin turns blue or purple — a change called cyanosis. The affected digits may ache or feel stiff during this phase. Cyanosis reflects deoxygenated blood pooling in the small vessels while arterial inflow remains restricted.
Red: The Reperfusion Phase
When the vasospasm releases and blood flow returns, the fingers flush a vivid red in the third phase. This reactive hyperaemia — meaning a rush of blood into previously starved tissue — causes throbbing, burning, and a painful tingling sensation. The return of colour marks the end of the attack, but discomfort can persist for several minutes afterward.
Primary vs Secondary Raynaud’s Phenomenon
Doctors classify Raynaud’s phenomenon into two distinct types based on whether an underlying condition is responsible. This distinction is clinically important because it influences both prognosis and management.
Primary Raynaud’s Phenomenon
Primary Raynaud’s phenomenon — also called Raynaud’s disease — occurs independently, without any associated underlying medical condition. It is by far the most common form, affecting approximately 3–5% of the general population in temperate climates. Primary Raynaud’s tends to cause milder, more symmetrical attacks and rarely leads to tissue damage.
Young women are most commonly affected, with symptoms typically beginning in adolescence or early adulthood. The exact mechanism remains incompletely understood, but abnormal nerve signalling and enhanced vascular sensitivity to cold appear to play central roles. Family history is common, suggesting a genetic contribution.
Secondary Raynaud’s Phenomenon
Secondary Raynaud’s phenomenon — called Raynaud’s syndrome — occurs as a consequence of an underlying disease or external trigger. This form is generally more severe, more asymmetrical, and carries a higher risk of complications including digital ulceration and tissue damage.
Secondary Raynaud’s typically presents in older individuals and warrants thorough investigation to identify the underlying cause. Unlike the primary form, it may progress to causing persistent pain and skin changes even between attacks.
Why the Distinction Matters
Distinguishing between primary and secondary Raynaud’s influences the clinical approach significantly. Primary Raynaud’s often requires only lifestyle modifications and occasionally mild medications. Secondary Raynaud’s demands investigation and treatment of the underlying condition, alongside targeted vascular therapies to protect the fingers and toes from ischaemic damage.
What Causes Secondary Raynaud’s Phenomenon?
Secondary Raynaud’s phenomenon arises from a broad range of underlying conditions, medications, and occupational or environmental exposures.
Autoimmune and Connective Tissue Diseases
Autoimmune conditions are the most important causes of secondary Raynaud’s phenomenon. Systemic sclerosis (scleroderma) carries the strongest association — Raynaud’s phenomenon affects virtually all people with this condition and often precedes other scleroderma features by years. Systemic lupus erythematosus (SLE), Sjögren’s syndrome, rheumatoid arthritis, dermatomyositis, and mixed connective tissue disease all frequently cause secondary Raynaud’s.
In these conditions, immune-mediated damage to small blood vessels and abnormal antibody production disrupt normal vascular function. Identifying these diseases early allows treatment to begin before irreversible vascular damage occurs.
Arterial and Vascular Diseases
Conditions that directly affect the arteries can precipitate Raynaud’s phenomenon. Atherosclerosis — fatty plaque buildup in artery walls — and Buerger’s disease, a vasculitis strongly linked to smoking, both impair peripheral circulation and trigger attacks. Thoracic outlet syndrome, where blood vessels are compressed between the collarbone and first rib, can also cause unilateral Raynaud’s features.
Occupational Triggers
Prolonged use of vibrating tools — such as jackhammers, drills, and chainsaws — causes a specific occupational form called vibration-induced white finger or hand-arm vibration syndrome (HAVS). Repeated vibration damages the blood vessels and nerves in the hands, causing persistent Raynaud’s-like attacks. Cold working environments further compound this risk.
Medications and Substances
Several medications can trigger or worsen Raynaud’s phenomenon by narrowing blood vessels. Beta-blockers used for heart disease and high blood pressure are common culprits. Certain migraine treatments, chemotherapy agents including bleomycin and vinblastine, decongestants containing pseudoephedrine, and ergotamine-containing medications all carry this risk.
Nicotine from smoking causes powerful vasoconstriction and worsens Raynaud’s attacks considerably. Cocaine use similarly provokes intense vasospasm and represents a preventable trigger.
Who Is Most at Risk?
Raynaud’s phenomenon affects a wide range of people, though certain characteristics raise individual risk significantly.
Age and Sex
Primary Raynaud’s predominantly affects young women, with most cases beginning between 15 and 30 years of age. Estimates suggest women develop primary Raynaud’s approximately nine times more often than men. Secondary Raynaud’s affects a broader age range, typically presenting after age 40 when underlying autoimmune conditions become more apparent.
Geographic and Environmental Factors
People living in colder climates experience Raynaud’s attacks more frequently and with greater severity than those in warmer regions. However, Raynaud’s phenomenon is not exclusively a cold-climate condition. Even in warm regions, air conditioning, refrigerated environments, and seasonal temperature swings trigger attacks in susceptible individuals.
Family History and Genetics
A family history of Raynaud’s phenomenon increases personal risk, supporting a genetic predisposition. Twin studies suggest that genetics contribute meaningfully to primary Raynaud’s susceptibility. Specific genetic variants affecting vascular reactivity and serotonin signalling pathways have been identified in research studies, though genetic testing is not yet part of routine clinical practice.
Recognising the Symptoms
Symptoms of Raynaud’s phenomenon extend beyond the visible colour changes, affecting sensation, function, and sometimes skin integrity.
Sensory Symptoms During an Attack
Numbness is one of the earliest sensations during a Raynaud’s attack as blood flow diminishes. Tingling, burning, and throbbing pain accompany the colour changes, particularly during the reperfusion phase when blood rushes back. Some people experience a feeling of tightness or swelling in the affected digits.
Between attacks, most people with primary Raynaud’s feel entirely normal. Secondary Raynaud’s may cause persistent discomfort, coldness, or sensitivity even outside of discrete attack episodes.
Which Body Parts Are Affected
Although the fingers are most commonly involved, Raynaud’s can affect the toes, ears, nose, lips, tongue, and nipples. Bilateral finger involvement — affecting both hands symmetrically — is typical of primary Raynaud’s. Asymmetrical involvement, or attacks affecting only one hand or one or two specific fingers, raises concern for secondary Raynaud’s and warrants further investigation.
Skin and Tissue Complications
In severe or prolonged secondary Raynaud’s, repeated episodes of poor blood supply can damage skin and underlying tissues. Digital pitting — small, depressed scars on fingertip skin — and digital ulcers, which are painful open sores at the fingertips, indicate significant ischaemic damage. Left untreated, severe digital ulcers can progress to gangrene in rare cases, particularly in scleroderma-related Raynaud’s.
How Doctors Diagnose Raynaud’s Phenomenon
Diagnosing Raynaud’s phenomenon rests primarily on clinical history and examination. No single laboratory test confirms the diagnosis, but investigations help distinguish primary from secondary disease.
Clinical History and Examination
A thorough clinical history captures the nature, frequency, duration, and triggers of colour change episodes. Doctors ask about symmetry, which digits are affected, family history, occupational exposures, medications, and symptoms suggesting autoimmune disease such as joint pain, dry eyes, or skin changes.
Physical examination looks for signs of underlying connective tissue disease, including puffy fingers, skin thickening, telangiectasias (small dilated blood vessels visible on skin), and nail fold capillary changes visible under a dermatoscope or ophthalmoscope.
Nailfold Capillaroscopy
Nailfold capillaroscopy is a key investigation that uses a magnifying instrument to examine the tiny capillaries at the base of fingernails. In primary Raynaud’s, the capillaries appear normal in number and structure. In secondary Raynaud’s associated with autoimmune diseases — particularly scleroderma — the capillaries show characteristic enlargement, dropout, and distortion called a scleroderma pattern.
This simple, non-invasive test powerfully discriminates primary from secondary Raynaud’s and directly guides further investigation.
Blood Tests for Underlying Conditions
Blood tests help identify autoimmune causes of secondary Raynaud’s. Antinuclear antibody (ANA) testing screens broadly for autoimmune conditions. Specific antibodies — including anti-centromere antibodies and anti-Scl-70 antibodies — suggest scleroderma. Anti-double-stranded DNA antibodies point toward lupus.
Inflammatory markers including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) detect systemic inflammation. A full blood count, thyroid function tests, and cryoglobulin testing round out the initial evaluation in suspected secondary Raynaud’s.
Cold Challenge Testing
Formal cold provocation testing — submerging hands in cold water and measuring finger temperature recovery time — can objectively document vasospastic responses. However, this test is primarily a research tool and is not routinely required for clinical diagnosis in most patients. It provides useful objective documentation in occupational or medicolegal contexts.
Managing Raynaud’s Phenomenon
Treatment aims to reduce attack frequency, relieve symptoms, protect the digits from damage, and address underlying causes in secondary disease.
Lifestyle Modifications
Avoiding cold exposure and sudden temperature changes forms the cornerstone of management for both types. Wearing warm gloves, layering clothing, and maintaining a warm environment reduce attack triggers considerably. Hand warmers and heated gloves offer practical protection during colder months.
Keeping the whole body warm — rather than just the hands — is particularly effective. Because Raynaud’s attacks can be triggered by a drop in core temperature, wearing warm hats, thermal socks, and insulated footwear helps prevent peripheral vasospasm even when hands are covered.
Reducing Stress Triggers
Emotional stress triggers vasospasm through the sympathetic nervous system, prompting blood vessel constriction independently of cold. Stress management strategies including mindfulness, meditation, yoga, and regular moderate exercise improve autonomic nervous system balance and may reduce attack frequency.
Identifying and managing psychological stressors alongside physical cold triggers provides a more comprehensive approach to Raynaud’s control.
Smoking Cessation
Stopping smoking is one of the most important interventions for people with Raynaud’s phenomenon. Nicotine constricts small blood vessels powerfully and reliably worsens both attack frequency and severity. Healthcare providers can offer pharmacological and behavioural support to assist with smoking cessation.
Medications for Raynaud’s Phenomenon
When lifestyle measures prove insufficient, several medications effectively reduce vasospasm and protect against digital complications.
Calcium Channel Blockers
Calcium channel blockers — particularly long-acting nifedipine — are the first-line pharmacological treatment for Raynaud’s phenomenon. These medications relax the smooth muscle in blood vessel walls, reducing vasospasm frequency and severity. Clinical evidence demonstrates that nifedipine significantly reduces both attack frequency and duration in both primary and secondary Raynaud’s.
Amlodipine offers a convenient once-daily alternative with good tolerability. Side effects including headache, flushing, and ankle swelling occur in some patients but generally improve with dose adjustment.
Phosphodiesterase-5 Inhibitors
Sildenafil and tadalafil — medications primarily known for treating erectile dysfunction and pulmonary arterial hypertension — also effectively reduce Raynaud’s attack severity by promoting blood vessel relaxation. These agents are particularly useful in secondary Raynaud’s associated with scleroderma and in patients who do not tolerate calcium channel blockers adequately.
Topical and Intravenous Therapies
Topical glyceryl trinitrate (GTN) cream applied to the base of affected fingers promotes local vasodilation and provides targeted relief. Intravenous iloprost — a prostacyclin analogue that powerfully dilates blood vessels — is reserved for severe secondary Raynaud’s with digital ulcers, particularly in scleroderma. Hospital infusions of iloprost reduce ulcer healing time and prevent new ulcer formation.
Treating Digital Ulcers
Active digital ulcers require specialist wound care, antibiotics if infection develops, and optimisation of vasodilatory therapy. Bosentan, an endothelin receptor antagonist, reduces new digital ulcer formation in scleroderma-related Raynaud’s. Surgical sympathectomy — cutting the nerves responsible for vasospasm — offers relief in selected severe cases unresponsive to medical therapy.
Living Well With Raynaud’s Phenomenon
Most people with primary Raynaud’s lead full, active lives with simple precautions and occasional medication. Managing secondary Raynaud’s requires greater vigilance but remains highly achievable with appropriate care.
Practical Daily Strategies
Keeping gloves and hand warmers readily accessible — in bags, coat pockets, and workplaces — allows rapid response when an attack begins. Warming affected hands gently under warm (not hot) water or placing them in the armpits rapidly reverses vasospasm. Swinging the arms in circular windmill motions generates centrifugal force that pushes blood back into the fingers.
Planning ahead for cold environments, avoiding direct contact with frozen foods without protective gloves, and requesting workplace adjustments for cold working conditions all reduce attack burden meaningfully.
Diet and Supplements
Some evidence suggests that fish oil supplementation may modestly reduce Raynaud’s attack severity by promoting vasodilation. Magnesium plays a role in vascular smooth muscle function, and adequate dietary intake supports healthy circulation. While no specific diet prevents Raynaud’s attacks, a heart-healthy diet rich in antioxidants supports overall vascular health.
Limiting caffeine — which promotes vasoconstriction — may reduce attack frequency in sensitive individuals.
Emotional Support and Community
Living with Raynaud’s phenomenon, particularly the secondary form associated with autoimmune diseases, can affect mental wellbeing significantly. Connecting with patient organisations such as the Raynaud’s Association or Scleroderma and Raynaud’s UK (SRUK) provides community support, practical advice, and access to updated medical information. Healthcare providers can offer referrals to counselling or support groups when psychological burden becomes significant.
Frequently Asked Questions
Is Raynaud’s phenomenon dangerous?
For most people with primary Raynaud’s, the condition is uncomfortable and inconvenient but not dangerous. It does not progress to causing permanent damage in the majority of cases. Secondary Raynaud’s carries greater risk, particularly when associated with scleroderma, where repeated episodes can cause digital ulcers and, rarely, tissue loss. Prompt identification of underlying conditions and appropriate treatment minimise these risks considerably.
Can Raynaud’s phenomenon go away on its own?
Primary Raynaud’s can improve over time, particularly as people learn to identify and avoid their specific triggers. Some younger women find that symptoms diminish in warmer seasons and with age. Secondary Raynaud’s rarely resolves entirely without treating the underlying condition. Effective management of the associated autoimmune disease can reduce attack severity significantly.
Does Raynaud’s phenomenon only affect the hands?
No — while the fingers are most commonly affected, Raynaud’s phenomenon can involve the toes, ears, nose, lips, tongue, and nipples. Nipple Raynaud’s is a recognised but often overlooked condition that causes significant pain, particularly in people who breastfeed. Recognising Raynaud’s involvement beyond the hands ensures comprehensive management of all affected sites.
What is the connection between Raynaud’s and scleroderma?
Raynaud’s phenomenon is nearly universal in scleroderma — a systemic autoimmune disease causing skin thickening, vascular damage, and internal organ fibrosis. Raynaud’s frequently precedes other scleroderma features by several years, making it an important early warning sign. Anyone developing Raynaud’s phenomenon after age 40, or with abnormal nailfold capillaries, should receive specialist evaluation to detect scleroderma at its earliest treatable stage.
Can children develop Raynaud’s phenomenon?
Yes, Raynaud’s phenomenon can affect children and adolescents, most commonly as the primary form. Teenage girls represent a commonly affected group, with symptoms often beginning around puberty. Children with Raynaud’s phenomenon should receive evaluation to exclude secondary causes, particularly autoimmune conditions, though primary disease is far more prevalent in this age group.
Are there any foods that help Raynaud’s phenomenon?
No single food cures or prevents Raynaud’s attacks, but dietary choices can support vascular health. Foods rich in omega-3 fatty acids — such as oily fish, flaxseeds, and walnuts — may promote vasodilation. Antioxidant-rich foods including berries, leafy greens, and colourful vegetables reduce oxidative stress in blood vessel walls. Avoiding or limiting caffeine and alcohol, both of which affect peripheral circulation, may help reduce attack frequency in some individuals.
Conclusion
Raynaud’s phenomenon is far more than fingers that feel the cold a little more than usual. For millions of people, it represents a daily negotiation with temperature, stress, and circulation — one that affects work, leisure, and quality of life in tangible ways. Understanding what happens during an attack, recognising the difference between primary and secondary forms, and knowing when to seek specialist care all make a meaningful difference.
The good news is that most people with Raynaud’s phenomenon — particularly the primary form — can manage their symptoms effectively with the right combination of lifestyle adjustments, trigger avoidance, and where necessary, medication. For those with secondary Raynaud’s, early diagnosis of the underlying condition opens the door to treatments that protect the fingers and preserve long-term function. Your circulation deserves attention, and Raynaud’s phenomenon is a condition worth taking seriously.
References
- Systemic sclerosis is a chronic autoimmune connective tissue disease characterized by skin fibrosis and often involving internal organs.
- Mixed Connective Tissue Disease has certain distinctive clinical and laboratory features that help differentiate it from other connective tissue diseases.
- MCTD presents with overlapping features from multiple autoimmune diseases.
Disclaimer:
This article is for general informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personalised diagnosis, treatment, or health guidance.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.