
Tuberculosis: The World’s Deadliest Infectious Disease Kills 1.23 Million Annually Despite Being Curable
KEY FACTS
- In 2024, tuberculosis killed 1.23 million people globally, including 150,000 among people with HIV, making it the world’s leading infectious disease killer
- An estimated 10.7 million people fell ill with TB worldwide in 2024, including 5.8 million men, 3.7 million women, and 1.2 million children
- Multidrug-resistant TB (MDR-TB) remains a public health crisis—only about 2 in 5 people with drug-resistant TB accessed treatment in 2024
- WHO reports that global efforts to combat TB have saved an estimated 83 million lives since 2000
- People living with HIV are 12 times more likely to develop TB disease than people without HIV, with TB the leading cause of death among HIV-positive individuals
On November 13, 2025, WHO released data revealing both progress and peril in the global fight against tuberculosis. For the first time since the COVID-19 pandemic, TB cases declined—dropping nearly 2% while deaths fell 3%. But here’s the sobering reality: TB still killed 1.23 million people in 2024, making it the deadliest infectious disease on the planet.
According to WHO’s Global Tuberculosis Report 2025 (https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/tb-reports/global-tuberculosis-report-2025), the disease remains “a major cause of deaths related to antimicrobial resistance” and continues as a top 10 cause of death globally. The $22 billion needed annually by 2027 to meet global targets? Only $5.9 billion materialized in 2024, leaving a funding gap that WHO Director-General Tedros Adhanom Ghebreyesus warns could “reverse the hard won gains.”
This article examines WHO’s framework on tuberculosis, the emergence of drug-resistant strains threatening decades of progress, and why a disease that’s both preventable and curable continues claiming lives at catastrophic rates—particularly within global health systems already strained by resource constraints.
What Is Tuberculosis? WHO’s Definition
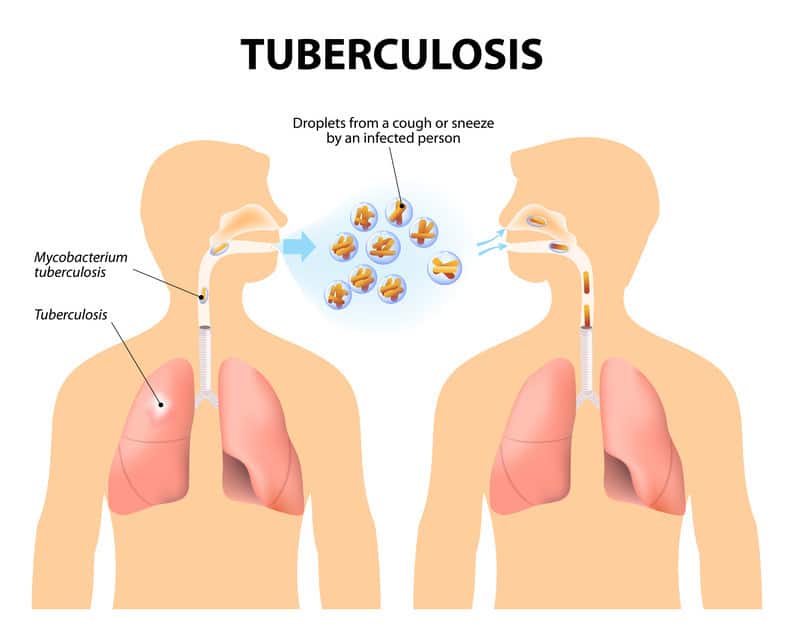
According to WHO’s fact sheet on tuberculosis (https://www.who.int/news-room/fact-sheets/detail/tuberculosis), TB is “an infectious disease caused by bacteria that most often affects the lungs.” The causative organism, Mycobacterium tuberculosis, spreads through the air when people with active pulmonary TB cough, sneeze, spit, or talk—releasing tiny droplets containing the bacteria.
But here’s what makes TB particularly insidious: not everyone infected develops active disease. Most people infected with TB bacteria carry what’s called latent TB infection—they’re not sick, can’t transmit the disease, but harbor dormant bacteria that can activate years later if their immune system weakens.
WHO distinguishes between these two states. Latent TB infection involves no symptoms and no contagion. Active TB disease causes illness and spreads to others. The transition between these states depends heavily on immune function—which is why HIV co-infection proves so deadly.
The bacteria primarily attack the lungs (pulmonary TB), but can also affect other parts of the body including kidneys, spine, and brain (extrapulmonary TB). Without treatment, WHO notes that people with active TB infect 5-15 others annually on average. Left untreated, active TB kills approximately half of those affected.
Global Burden: Who’s Most at Risk?
WHO’s 2024 data reveals a disease burden that defies its curable status. An estimated 10.7 million people fell ill with TB globally in 2024—comprising 5.8 million men, 3.7 million women, and 1.2 million children. Of those, 1.23 million died, including 150,000 people with HIV.
Geographic concentration tells a stark story. Just five countries—China, India, Indonesia, Pakistan, and the Philippines—accounted for more than half of global TB cases in 2024, according to WHO’s Global TB Report. Thirty countries combined represented 87% of the global total. Research published in medical journals analyzing the 2024 WHO data (https://pmc.ncbi.nlm.nih.gov/articles/PMC11995120/) found that “over 80% of cases and deaths are in low- and middle-income countries.”
Drug-resistant TB presents an escalating crisis within the crisis. WHO estimates approximately 410,000 people developed multidrug-resistant or rifampicin-resistant TB (MDR/RR-TB) globally, yet only about 2 in 5 accessed treatment. The treatment success rate for MDR-TB reached 68% in 2020—up from 50% in 2012—but remains “alarmingly low” according to WHO assessments.
HIV co-infection multiplies vulnerability dramatically. WHO data shows people living with HIV are 12 times more likely to develop TB disease than HIV-negative individuals. In 2024, approximately 150,000 people died of HIV-associated TB, with the WHO African Region bearing the highest burden. Yet globally, only 61% of HIV-positive people who developed TB received antiretroviral therapy.
Socioeconomic factors WHO identifies as driving TB transmission include:
- Undernutrition (responsible for an estimated 970,000 new TB cases in 2024)
- Diabetes (930,000 new cases)
- Alcohol use disorders (740,000 cases)
- Smoking (700,000 cases)
- HIV infection (570,000 cases)
CDC surveillance data from the United States (https://www.cdc.gov/tb-surveillance-report-2024/index.html) provides context for high-resource settings. In 2024, the US reported 10,388 TB cases with an incidence rate of 3.1 per 100,000 population—representing a 7.9% increase from 2023 and the highest level in over a dozen years. California, Texas, New York, and Florida accounted for half of all US cases.
WHO reports that “TB mostly affects adults in their most productive years,” though all age groups face risk. Catastrophically, about 50% of people treated for TB and their households face costs exceeding 20% of total household income—far from the WHO End TB Strategy target of zero.
Causes, Transmission & Risk Factors
Tuberculosis spreads through a deceptively simple mechanism: airborne transmission of Mycobacterium tuberculosis bacteria. When a person with active pulmonary TB releases bacteria into the air, others in close proximity can inhale them. WHO emphasizes that TB is “contagious and airborne”—a single untreated person can infect 5-15 others annually.
But infection doesn’t equal disease. According to WHO’s transmission framework, several factors determine whether exposure leads to active TB:
Immune system status: People with compromised immunity face dramatically elevated risk. WHO identifies specific vulnerability groups:
- HIV-positive individuals (12 times higher risk than HIV-negative people)
- Individuals receiving immunosuppressive therapy (tumor necrosis factor-alpha inhibitors, solid organ transplant recipients)
- People with diabetes
- Those with undernutrition
- Tobacco users
- Alcohol users
Environmental factors documented by WHO include:
- Overcrowded living conditions facilitating airborne transmission
- Poor ventilation in homes, workplaces, or congregate settings
- Poverty limiting access to healthcare
- Food insecurity and malnutrition weakening immune response
Drug resistance emergence poses unique transmission risks. WHO reports that “the two reasons why MDR/RR-TB continues to emerge and spread are mismanagement of TB treatment and person-to-person transmission.” According to WHO guidelines (https://www.who.int/news-room/questions-and-answers/item/tuberculosis-multidrug-resistant-tuberculosis-(mdr-tb)), “inappropriate or incorrect use of TB drugs, use of ineffective formulations of drugs (such as the use of single drugs, poor quality medicines or bad storage conditions), and premature treatment interruption can cause drug resistance, which can then be transmitted, especially in crowded settings such as prisons and hospitals.”
Research examining TB transmission patterns found that CDC molecular surveillance data (https://www.cdc.gov/tb-surveillance-report-2024/data/cases-in-large-outbreaks.html) identified six large outbreaks in the US in 2024 involving 129 total cases, with approximately 53% occurring in US-born persons—demonstrating ongoing domestic transmission despite low overall incidence.
The bacteria’s resilience compounds transmission risk. M. tuberculosis can survive for hours in the air and withstand many disinfectants. Only direct sunlight and good ventilation reliably reduce airborne concentration. This durability explains why TB thrives in crowded, poorly ventilated settings—from prisons to refugee camps to urban slums.
Signs, Symptoms and Health Impacts
WHO identifies a spectrum of manifestations ranging from asymptomatic latent infection to life-threatening active disease. The clinical presentation varies dramatically between pulmonary and extrapulmonary TB.
Pulmonary TB symptoms WHO documents include:
- Persistent cough lasting three weeks or longer (often producing blood-tinged sputum)
- Chest pain
- Weakness or fatigue
- Weight loss
- Fever
- Night sweats
- Loss of appetite
But here’s what complicates diagnosis: these symptoms develop gradually and can mimic other respiratory conditions. WHO emphasizes that many people delay seeking care, allowing disease progression and continued transmission. Research shows the average TB patient remains infectious for weeks to months before diagnosis.
Extrapulmonary TB can affect virtually any organ system, WHO notes. Common sites include:
- Lymph nodes (most frequent extrapulmonary manifestation)
- Pleura (lining of lungs)
- Genitourinary system
- Bones and joints
- Meninges (brain and spinal cord covering)
- Abdomen
Central nervous system TB proves particularly deadly. TB meningitis carries high mortality even with treatment, and survivors often face permanent neurological damage.
HIV co-infection dramatically alters disease presentation. CDC clinical guidance notes that HIV-positive individuals more frequently develop extrapulmonary TB, disseminated disease, and atypical chest X-ray findings that can delay diagnosis.
Long-term health impacts WHO identifies include:
- Permanent lung damage from pulmonary TB
- Chronic respiratory impairment
- Increased cardiovascular disease risk
- Neurological sequelae from TB meningitis
- Skeletal deformity from bone TB
- Reproductive complications from genitourinary TB
Drug-resistant TB creates additional health burdens. Treatment requires longer duration (up to 24 months versus 6 months for drug-susceptible TB), more toxic medications, and carries higher failure rates. WHO reports that adverse events from second-line TB drugs include hearing loss, peripheral neuropathy, psychiatric symptoms, and kidney damage.
Socioeconomic health impacts extend beyond physical illness. WHO data shows approximately 50% of TB-affected households face catastrophic costs, forcing families into poverty through medical expenses and lost income during lengthy treatment. The psychological burden—stigma, discrimination, treatment fatigue—compounds physical suffering.
Similar to collaborative approaches seen in Indian TB elimination efforts, addressing TB’s full health impact requires integrating medical treatment with social support systems.
Treatment and Health Response
WHO reports fundamental shifts in TB treatment protocols over recent years, particularly for drug-resistant cases. The standard treatment approach varies dramatically by drug-susceptibility status.
Drug-susceptible TB treatment follows WHO’s recommended 6-month regimen comprising four first-line drugs: isoniazid, rifampicin, ethambutol, and pyrazinamide. Most people are cured by this regimen when provided with adequate support, WHO notes. Treatment success requires direct observation—healthcare workers or trained community members watch patients take medications to ensure adherence.
Drug-resistant TB treatment underwent revolutionary changes with WHO’s December 2022 guidelines (https://www.who.int/publications/i/item/9789240063129). The breakthrough: a 6-month all-oral regimen called BPaLM, composed of bedaquiline, pretomanid, linezolid, and moxifloxacin.
According to WHO’s landmark announcement (https://www.who.int/news/item/15-12-2022-who-announces-landmark-changes-in-treatment-of-drug-resistant-tuberculosis), “The newly recommended BPaLM regimen offers better outcomes, remarkably shortens the duration of treatment, and thus significantly improves quality of life for people with MDR/RR-TB.” The previous standard required 18-24 months of treatment with injectable agents causing severe side effects including permanent hearing loss.
WHO data shows rapid BPaLM uptake: globally in 2024, approximately 34,000 people with MDR/RR-TB started treatment on 6-month shorter regimens (BPaLM and BDLLfxC)—a substantial increase from 5,653 in 2023 and 1,744 in 2022. Forty countries had implemented BPaLM by end of 2022.
CDC treatment guidelines (https://www.cdc.gov/tb/hcp/treatment/drug-resistant-tuberculosis-disease.html) for the United States align with WHO recommendations, offering BPaLM for eligible patients aged 14 and older with rifampin-resistant, fluoroquinolone-susceptible pulmonary TB.
Access barriers WHO identifies remain severe:
- Only about 2 in 5 people with drug-resistant TB accessed treatment in 2024
- Treatment costs remain high (≥$1,000 per person for MDR-TB versus <$100 for drug-susceptible TB)
- Drug stockouts and supply chain failures disrupt treatment in resource-limited settings
- Insufficient laboratory capacity for drug-susceptibility testing delays appropriate regimen selection
- Healthcare worker shortages limit treatment supervision capacity
Regional differences in treatment access prove stark. Research analyzing WHO’s 2024 data found that while treatment success rates for MDR-TB reached 71% globally in recent cohorts, many high-burden countries struggle to diagnose and initiate treatment for even half of estimated cases.
WHO emphasizes that “most people with TB are cured by a 6-month treatment regimen that is provided to patients with adequate support”—yet achieving that support requires health system investments many countries can’t afford.
Prevention & WHO Strategies
WHO’s prevention framework operates on multiple levels, from individual prophylaxis to population-wide interventions. The centerpiece: the Bacillus Calmette-Guérin (BCG) vaccine, though its limitations shape broader prevention strategies.
BCG vaccination WHO recommends for all infants in countries with high TB burden. The vaccine protects against severe forms of TB in children—particularly TB meningitis and disseminated disease—but provides variable protection against pulmonary TB in adolescents and adults. WHO notes that BCG remains the world’s most widely used vaccine, administered to over 100 million infants annually.
Preventive treatment for latent TB infection represents WHO’s priority prevention intervention. According to WHO guidelines, people at high risk—including household contacts of TB patients, people living with HIV, and individuals with certain medical conditions—should receive preventive therapy to stop progression from latent infection to active disease.
WHO recommends several preventive regimens:
- Daily isoniazid for 6 or 9 months
- Weekly isoniazid plus rifapentine for 3 months (3HP regimen)
- Daily rifampicin for 4 months
Data shows that preventive treatment reduces TB disease risk by 60-90% in eligible populations. Yet WHO reports persistent gaps in implementation—only a fraction of eligible individuals globally receive preventive therapy.
Infection control measures WHO emphasizes include:
- Rapid diagnosis and treatment of active cases to reduce transmission period
- Respiratory etiquette (cough hygiene) in healthcare settings and communities
- Environmental controls (ventilation, ultraviolet germicidal irradiation) in high-risk facilities
- Administrative controls limiting exposure in congregate settings
Addressing social determinants WHO identifies as essential to prevention:
- Reducing household overcrowding
- Improving nutrition and food security
- Reducing tobacco and alcohol use
- Expanding HIV prevention and treatment
- Enhancing diabetes screening and management
Efforts paralleling tuberculosis elimination partnerships demonstrate how multi-sectoral collaboration amplifies prevention impact beyond healthcare alone.
Emerging prevention tools in WHO’s development pipeline include:
- New TB vaccines showing promise in clinical trials
- Shorter preventive treatment regimens
- Point-of-care diagnostics enabling same-day treatment initiation
- Digital adherence technologies improving treatment completion
WHO’s End TB Strategy sets ambitious prevention targets: 90% of household contacts and other high-risk groups receiving preventive treatment, 90% of people living with HIV receiving TB preventive therapy, and universal health coverage eliminating catastrophic costs for TB-affected families.
WHO’s Global Efforts and Recent Developments
WHO’s tuberculosis elimination work has intensified against a backdrop of both promising innovation and troubling setbacks. The organization’s Global TB Programme coordinates response across 184 countries reporting data in 2025.
The 2023 UN High-Level Meeting on TB established new targets requiring $22 billion annually for TB prevention, diagnosis, treatment, and care by 2027. Yet WHO’s November 2025 report reveals only $5.9 billion became available in 2024—just over one quarter of the target. Research and development funding proved similarly inadequate: $1.2 billion raised versus a $5 billion annual target.
WHO’s End TB Strategy milestones for 2025 aimed for a 75% reduction in TB deaths and 50% reduction in incidence compared to 2015 levels. The November 2025 data (https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/tb-reports/global-tuberculosis-report-2025/tb-disease-burden/1-2-tb-mortality) shows the global community falling dramatically short: only a 29% reduction in deaths and 12% reduction in incidence achieved between 2015-2024.
November 13, 2025 WHO Global TB Report marks a pivotal moment—the first decline in TB cases since COVID-19 disruptions. WHO Director-General Tedros stated: “The data show that global efforts are beginning to turn the tide, with the TB burden and death declining for the first time since the COVID-19 pandemic.” But he cautioned: “Progress is not victory. The fact that TB continues to claim over a million lives each year, despite being preventable and curable, is simply unconscionable.”
Regional progress varies wildly. WHO’s African Region achieved a 28% reduction in TB incidence and 46% reduction in deaths from 2015-2024. Europe reached 39% and 49% reductions respectively. But other regions lag far behind, with COVID-19 pandemic disruptions setting back years of progress.
December 2022 treatment guideline revolution represented WHO’s most significant recent breakthrough. The BPaLM regimen approval (https://www.who.int/news/item/15-12-2022-who-announces-landmark-changes-in-treatment-of-drug-resistant-tuberculosis) transformed MDR-TB treatment from 18-24 month injectable-based torture to 6-month all-oral regimens with better outcomes.
December 31, 2024 joint clinical guideline update from ATS/CDC/ERS/IDSA further refined treatment protocols, offering patients shorter, safer, more effective regimens with fewer pills and injections. CDC noted the update represents “one of collaboration, progress, and shared commitment to eliminating TB.”
WHO’s surveillance innovations include molecular epidemiology networks tracking transmission patterns and drug resistance emergence. Research on SARS-CoV-2 and TB overlap through genomic surveillance demonstrates how pandemic-era tools strengthen TB response capacity.
But here’s WHO’s uncomfortable reality: recent progress faces existential threats. The dismantling of USAID by the Trump administration eliminated roughly one-third of international TB funding. Studies suggest wealthy-country funding cuts could lead to 2 million additional TB deaths and 10 million new illnesses over the next decade.
WHO’s Tereza Kasaeva, director of HIV/TB programs, acknowledged both the achievement and the peril: “The progress is still far short of meeting global targets, so it’s fairly clear we need to do significantly more.” The $16 billion funding gap between availability and need represents not just numbers—it’s treatment denied, lives lost, and drug resistance spreading unchecked.
Similar to patterns seen across historical health crises, the gap between technical capacity and political will determines outcomes. WHO has proven TB is curable—6-month drug-susceptible treatment, 6-month MDR-TB treatment, preventive therapy that works. What WHO can’t cure is the funding apathy that leaves millions without access to medicines that cost less than a smartphone.
As the November 2025 report makes clear: the decline in TB cases and deaths is real, but fragile. Without sustained funding and intensified effort, WHO warns the progress could vanish as quickly as it appeared—returning the world to the devastating trajectory COVID-19 disruptions created. Much like awareness campaigns for conditions such as cancer, TB elimination requires sustained political attention and resources, not cyclical interest that fades when headlines move on.
FAQ
According to WHO, TB spreads through the air when people with active pulmonary TB cough, sneeze, spit, or talk, releasing bacteria-containing droplets. Others nearby can inhale these droplets and become infected. TB is not transmitted through shaking hands, sharing food or drink, touching surfaces, or kissing. Only people with active TB disease in the lungs or throat can spread the infection; those with latent TB infection cannot transmit bacteria to others.
WHO reports that MDR-TB bacteria resist at least isoniazid and rifampicin, the two most powerful first-line TB drugs. Treatment requires second-line drugs that are more expensive (≥$1,000 per person versus <$100 for drug-susceptible TB), cause more severe side effects including permanent hearing loss, and require much longer duration—historically 18-24 months, though new BPaLM regimens reduced this to 6 months. Globally, only 2 in 5 people with drug-resistant TB accessed treatment in 2024, and success rates remain lower than for drug-susceptible TB.
WHO recommends BCG vaccination for all infants in high TB-burden countries. The vaccine protects against severe forms of TB in children, particularly TB meningitis and disseminated disease, but provides variable protection against pulmonary TB in adolescents and adults. BCG remains the world’s most widely used vaccine, administered to over 100 million infants annually. For people at high risk with latent TB infection, WHO recommends preventive treatment regimens that reduce disease development risk by 60-90%.
WHO data shows people living with HIV are 12 times more likely to develop TB disease than HIV-negative individuals. HIV weakens the immune system, making it harder to control TB bacteria. TB is the leading cause of death among people with HIV, causing approximately 150,000 deaths in 2024. HIV and TB form what WHO calls “a lethal combination, each accelerating the other’s progress.” Yet only 61% of HIV-positive people who developed TB received antiretroviral therapy globally in 2024.
According to WHO, TB is both preventable and curable. Most people with drug-susceptible TB are cured by a 6-month treatment regimen comprising four first-line drugs when provided with adequate support. For drug-resistant TB, WHO’s 2022 guidelines prioritized a 6-month all-oral BPaLM regimen offering better outcomes than previous 18-24 month injectable-based regimens. Global efforts to combat TB have saved an estimated 83 million lives since 2000. However, treatment success requires completion of the full regimen under supervision, and access gaps mean many who need treatment don’t receive it.
Sources
- World Health Organization. (2025). Tuberculosis (TB) Fact Sheet. https://www.who.int/news-room/fact-sheets/detail/tuberculosis
- World Health Organization. (2025). Global Tuberculosis Report 2025. https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/tb-reports/global-tuberculosis-report-2025
- World Health Organization. (2022). WHO consolidated guidelines on tuberculosis. Module 4: treatment – drug-resistant tuberculosis treatment, 2022 update. https://www.who.int/publications/i/item/9789240063129
- Centers for Disease Control and Prevention. (2025). Reported Tuberculosis in the United States, 2024. https://www.cdc.gov/tb-surveillance-report-2024/index.html
- Centers for Disease Control and Prevention. (2025). Treatment for Drug-Resistant Tuberculosis Disease. https://www.cdc.gov/tb/hcp/treatment/drug-resistant-tuberculosis-disease.html
DISCLAIMER
This article adapts publicly available information from WHO’s Tuberculosis page and related health organizations. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform—not a healthcare provider. For medical concerns related to tuberculosis, consult qualified healthcare professionals and follow guidance from local health authorities and TB programs.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.