
Benign Prostatic Hyperplasia: The Enlarged Prostate Explained
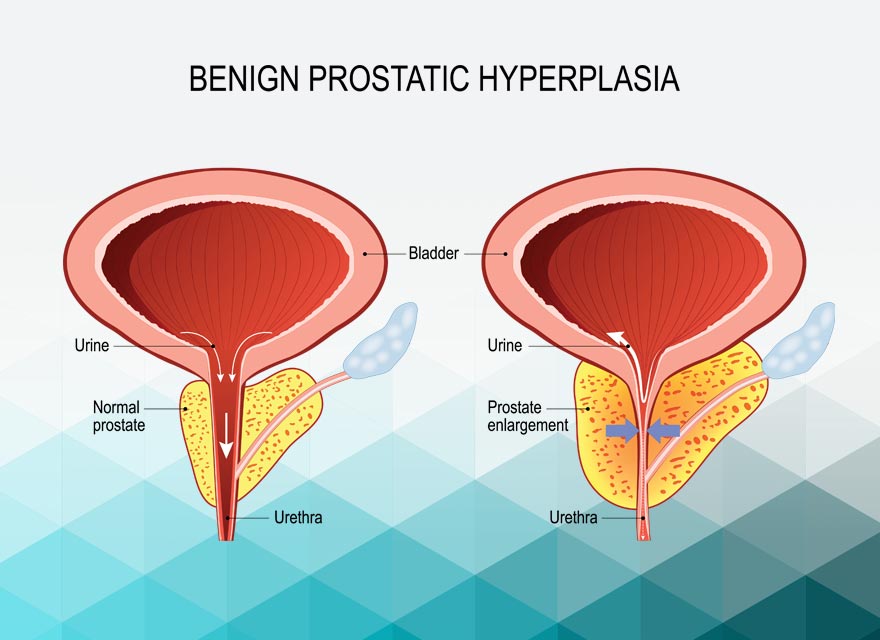
The prostate is a small gland — roughly the size of a walnut — that sits just below the bladder in people assigned male at birth. It wraps around the urethra, the tube that carries urine from the bladder out of the body. For most of life, this arrangement works smoothly. However, as the prostate grows larger with age, it begins to press on the urethra and makes urination increasingly difficult.
Benign prostatic hyperplasia — commonly called BPH — is the medical term for a prostate gland that has grown larger than normal. The word “benign” means non-cancerous. “Hyperplasia” means overgrowth of cells. BPH is therefore a non-cancerous enlargement of the prostate driven by the normal ageing process. It is not prostate cancer and it does not increase the risk of cancer developing.
Benign prostatic hyperplasia enlarged prostate treatment is one of the most relevant health topics for older men worldwide. BPH affects roughly 50% of men between the ages of 51 and 60 and up to 90% of men over 80. Furthermore, the urinary symptoms it causes — difficulty starting urination, weak flow, frequent nighttime trips to the bathroom — significantly affect sleep, comfort, and daily quality of life. Consequently, understanding BPH clearly and knowing when to seek treatment gives patients the confidence to act and the knowledge to choose the right care.
Quick Answer
Benign prostatic hyperplasia — BPH — is a non-cancerous enlargement of the prostate gland that occurs naturally with age. It presses on the urethra and causes urinary symptoms including weak flow, urgency, and frequent urination. Treatment ranges from lifestyle changes and medication to minimally invasive procedures and surgery depending on symptom severity.
What Is the Prostate and Why Does It Enlarge?
The Prostate’s Normal Role
The prostate gland has two main functions. First, it produces fluid that forms part of semen — nourishing and protecting sperm during ejaculation. Second, its position around the urethra means it plays an indirect role in controlling urinary flow. In a young adult, the prostate weighs roughly 20 grams — about the size of a walnut — and causes no urinary problems.
However, the prostate continues to grow throughout life in response to male hormones — particularly a form of testosterone called dihydrotestosterone, or DHT. This growth accelerates after the age of 40 in most men. By the time a man reaches his fifties or sixties, this growth often becomes significant enough to narrow the urethra and restrict urine flow. As a result, the bladder must work harder to push urine past the tightened outlet — and urinary symptoms begin.
Why Cells Multiply in BPH
In BPH, the cells of the inner part of the prostate gland — called the transition zone, which directly surrounds the urethra — multiply abnormally. This multiplication is driven primarily by DHT and by age-related changes in the balance between male and female hormones. Moreover, growth factors — chemical signals that stimulate cell division — play an increasingly recognised role in driving prostatic enlargement.
Importantly, this cell overgrowth is benign. It does not invade surrounding tissue or spread to other parts of the body the way cancer does. However, the physical consequences of a larger prostate pressing on the urethra are real, progressive, and in some cases serious if left unmanaged. For context on how urinary conditions can affect kidney health over time, see our article on chronic kidney disease — stages, symptoms, and how to slow the decline.
Symptoms of Benign Prostatic Hyperplasia
Lower Urinary Tract Symptoms
Benign prostatic hyperplasia enlarged prostate treatment begins with recognising the symptoms. BPH causes what doctors call lower urinary tract symptoms — or LUTS. These symptoms fall into two categories — obstructive and irritative — reflecting the two ways that an enlarged prostate affects bladder function.
Obstructive symptoms result directly from the prostate pressing on and narrowing the urethra. These include a weak or slow urinary stream, difficulty starting urination — called hesitancy — a stream that stops and starts, a feeling that the bladder has not fully emptied after urinating, and dribbling at the end of urination. Furthermore, straining to urinate is common as the bladder tries to generate extra pressure to push urine through the narrowed outlet.
Irritative Symptoms
Irritative symptoms result from the bladder responding to the increased outflow resistance. Over time, the bladder wall thickens and becomes overactive — contracting too frequently and with too much urgency. As a result, urinary frequency — needing to urinate more than eight times a day — and urinary urgency — a sudden and compelling need to urinate immediately — become prominent.
Nocturia — waking from sleep one or more times during the night to urinate — is one of the most disruptive symptoms of BPH. It significantly affects sleep quality, daytime energy levels, and overall wellbeing. Moreover, in severe cases, the bladder may not empty at all — a dangerous condition called acute urinary retention — which constitutes a medical emergency requiring immediate catheter drainage.
Symptoms overlap significantly with other conditions including interstitial cystitis and overactive bladder. For further reading on bladder conditions that produce similar symptoms, see our article on interstitial cystitis — the chronic condition behind UTI symptoms.
How Doctors Diagnose BPH
Initial Assessment
Diagnosing benign prostatic hyperplasia enlarged prostate treatment suitability begins with a careful clinical assessment. Doctors take a detailed history of urinary symptoms — asking about their duration, severity, and impact on daily life. The International Prostate Symptom Score — called IPSS — is a validated questionnaire that quantifies symptom severity on a scale from zero to 35. Scores below eight indicate mild symptoms, eight to nineteen indicate moderate symptoms, and twenty or above indicate severe symptoms.
Physical examination includes a digital rectal examination — called a DRE — in which the doctor gently inserts a gloved finger into the rectum to feel the back surface of the prostate. This allows assessment of prostate size, shape, and consistency. A smooth, rubbery, uniformly enlarged prostate suggests BPH. An irregular, hard, or nodular prostate raises concern for prostate cancer and requires further investigation. Furthermore, abdominal examination checks for a distended bladder that has not emptied fully.
Laboratory and Imaging Tests
Urine dipstick and urine culture tests exclude urinary tract infection as a contributing cause of symptoms. Blood tests measure renal function — including serum creatinine and eGFR — to assess whether the blocked outflow has affected the kidneys. For context on how urinary obstruction relates to kidney function, see our article on nephrotic syndrome — what protein in the urine actually tells you.
Prostate-specific antigen — called PSA — is a protein produced by prostate cells. A blood test measuring PSA levels helps exclude prostate cancer alongside the DRE finding. However, PSA can be elevated in BPH without cancer being present. Consequently, doctors interpret PSA results alongside clinical findings rather than in isolation.
Post-void residual measurement — using ultrasound to measure how much urine remains in the bladder after urinating — assesses how effectively the bladder empties. A large residual volume indicates significant obstruction. Moreover, uroflowmetry — measuring the speed and pattern of urine flow — objectively quantifies the degree of urethral obstruction. Consequently, combining symptom scores, physical findings, and flow measurements gives doctors a complete picture of disease severity before deciding on treatment.
Treatment of Benign Prostatic Hyperplasia
Watchful Waiting
Not all men with BPH need immediate treatment. Men with mild symptoms and no complications are often suitable for watchful waiting — also called active surveillance. This approach involves regular monitoring of symptoms, urine flow, and bladder function without starting medication or surgery. Meanwhile, lifestyle modifications form the foundation of this strategy.
Lifestyle changes include reducing fluid intake in the evening to minimise nocturia, limiting caffeine and alcohol — both of which irritate the bladder — and practising double voiding — urinating, waiting a few moments, then trying again to empty the bladder more completely. Furthermore, avoiding cold weather exposure and managing constipation reduce the pressure on the bladder and prostate. Consequently, many men with mild BPH manage their symptoms effectively through these simple adjustments alone for years.
Medications for BPH
When symptoms progress beyond the mild range, medication is the next step. Two main classes of drugs treat BPH effectively. Alpha-blockers — including tamsulosin, alfuzosin, and doxazosin — relax the smooth muscle in the prostate and bladder neck, reducing the resistance to urine flow. They work quickly — often producing noticeable improvement within one to two weeks. However, they do not reduce prostate size.
Five-alpha reductase inhibitors — including finasteride and dutasteride — block the conversion of testosterone to DHT, the hormone that drives prostate growth. They gradually reduce prostate volume over three to six months. Moreover, they significantly reduce the long-term risk of acute urinary retention and the need for surgery. However, they take longer to produce symptom relief than alpha-blockers.
Combining an alpha-blocker and a 5-alpha reductase inhibitor produces greater symptom relief than either drug alone in men with significantly enlarged prostates. In addition, PDE5 inhibitors — medications originally developed for erectile dysfunction, particularly tadalafil — have demonstrated effectiveness for BPH-related lower urinary tract symptoms and are now approved for this indication in several countries. Consequently, medication choice is tailored to the individual’s symptom pattern, prostate size, and personal preferences.
Minimally Invasive Procedures
For men who do not respond adequately to medication or who prefer a more definitive treatment without major surgery, several minimally invasive procedures are available. Rezum water vapour therapy uses steam delivered directly into prostate tissue to destroy excess cells, reducing prostate volume over several weeks. The UroLift system uses small implants placed through a cystoscope — a thin camera inserted through the urethra — to hold enlarged prostate tissue away from the urethra, immediately widening the urinary channel without removing tissue.
Both procedures have the advantage of preserving sexual function in the majority of patients — an important consideration for many men. Furthermore, both produce durable symptom improvement with a lower risk profile than surgical options. Consequently, minimally invasive procedures have become increasingly popular as first-choice interventions for moderate BPH in men who want to avoid long-term medication.
Surgical Treatment
Surgery remains the most effective and durable treatment for severe BPH or cases complicated by urinary retention, recurrent infections, bladder stones, or kidney damage. Transurethral resection of the prostate — called TURP — is the standard surgical procedure. A surgeon inserts a thin instrument through the urethra and removes the overgrown inner portion of the prostate using electrical current, creating a wider channel for urine to flow. TURP produces excellent and long-lasting symptom relief in the majority of patients.
Laser surgery — including holmium laser enucleation of the prostate, called HoLEP — offers an alternative to TURP with less bleeding and a shorter hospital stay. It is particularly suitable for very large prostates. Furthermore, open or robotic simple prostatectomy — surgically removing the inner part of the prostate through an incision or keyhole approach — is reserved for the largest prostates not suitable for endoscopic surgery. For broader context on how obstructive urinary conditions can contribute to kidney damage, see our article on kidney stones — types, causes, prevention, and pain management, and our article on focal segmental glomerulosclerosis and kidney failure.
Living Well With BPH
Long-Term Management and Monitoring
BPH is a progressive condition in most men. Even with treatment, regular monitoring is important to detect symptom worsening, medication side effects, or complications such as urinary retention, urinary tract infections, or bladder stones. Annual review with a doctor — including symptom score assessment, post-void residual measurement, and PSA monitoring — allows timely adjustment of the management plan.
Men taking 5-alpha reductase inhibitors should be aware that these medications reduce PSA levels by approximately 50% over time. Consequently, doctors must account for this reduction when interpreting PSA tests for cancer screening purposes. Furthermore, men who experience any sudden change in symptoms — particularly sudden inability to urinate, new blood in the urine, or worsening kidney function — need prompt medical review rather than waiting for a scheduled appointment.
Psychological and Relationship Impact
The urinary symptoms of BPH significantly affect quality of life beyond the purely physical. Nocturia disrupts sleep and causes daytime fatigue. Urgency and frequency restrict social activities, travel, and exercise. Moreover, concerns about sexual function — which some BPH medications and procedures can affect — deserve open discussion with the healthcare team.
Many men find it difficult to discuss urinary problems and consequently delay seeking help for years. This delay allows symptoms to worsen and increases the risk of complications including acute urinary retention and kidney damage. Therefore, open and non-judgemental conversations between patients and healthcare providers about urinary health are essential for achieving timely diagnosis and effective management.
When to Seek Urgent Medical Help
Seek emergency medical care immediately if you are unable to urinate at all — a condition called acute urinary retention. This is painful, distressing, and requires immediate bladder drainage with a catheter in a hospital setting. Furthermore, seek prompt medical attention if you notice blood in the urine, severe pain, high fever with urinary symptoms, or a significant sudden worsening of urinary flow.
In addition, any man with BPH who develops swollen ankles, reduced urine output, or elevated creatinine on blood tests needs urgent kidney function assessment to exclude obstruction-related kidney damage. Consequently, recognising these warning signs and acting promptly protects both bladder function and long-term kidney health.
Frequently Asked Questions
1. Is BPH the same as prostate cancer?
No. BPH and prostate cancer are completely different conditions. BPH is a non-cancerous enlargement of the prostate caused by normal cell overgrowth with ageing. Prostate cancer involves the uncontrolled growth of malignant cells that can spread to other parts of the body. Furthermore, having BPH does not increase the risk of developing prostate cancer. However, both conditions can produce similar urinary symptoms, which is why doctors assess for cancer during BPH evaluation.
2. At what age does BPH typically start?
Prostate enlargement begins in most men after the age of 40 but typically does not cause noticeable symptoms until the fifties or sixties. By age 60, roughly half of all men have some degree of BPH. By age 80, the proportion rises to approximately 90%. However, not all men with an enlarged prostate develop significant urinary symptoms — the relationship between prostate size and symptom severity varies considerably between individuals.
3. Can BPH be prevented?
There is no proven way to prevent BPH entirely because it is driven primarily by age-related hormonal changes. However, maintaining a healthy weight, exercising regularly, eating a balanced diet low in saturated fat and red meat, and limiting alcohol and caffeine may reduce the risk of developing severe symptoms. Moreover, regular medical check-ups allow early detection of prostate enlargement before complications develop. Consequently, a healthy lifestyle supports overall urological and kidney health throughout life.
4. Do BPH medications affect sexual function?
Some BPH medications do affect sexual function. Alpha-blockers can cause retrograde ejaculation — where semen enters the bladder instead of leaving the body during orgasm. Five-alpha reductase inhibitors can reduce libido and cause erectile dysfunction in a minority of patients. Furthermore, some surgical procedures also carry risks to sexual function. Consequently, discussing these potential effects openly with a doctor before starting treatment allows informed decision-making based on individual priorities.
5. Can BPH damage the kidneys?
Yes, if left untreated and severe. Chronic urinary obstruction from BPH increases pressure within the bladder and can eventually cause urine to back up into the kidneys — a condition called hydronephrosis — leading to kidney damage over time. Moreover, repeated urinary tract infections secondary to incomplete bladder emptying also threaten kidney health. Consequently, treating BPH effectively before obstruction becomes severe is an important way to protect long-term kidney function. For more information on how kidney function is assessed and protected, see our article on chronic kidney disease — stages, symptoms, and how to slow the decline.
References
- Black men face significantly higher prostate cancer risk—both higher rates of diagnosis and higher rates of dying from the disease
- BRCA mutations, we need to understand BRCA gene function and how mutations increase cancer risk.
- The Gleason scoring system, while medically useful, creates problems for patient understanding.
- Bladder cancer predominantly affects older adults and men.
- Kidney stones are hard mineral deposits that form inside the kidneys when certain substances in the urine become too concentrated.
Disclaimer
This article adapts publicly available information from WHO’s Noncommunicable Diseases page. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform and not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.