
Age-Related Macular Degeneration (AMD): Dry vs Wet — Treatment Options for Each
Reading a book, recognising a face, watching a sunset — all of these experiences depend on the macula, a tiny but critical region at the centre of the retina. When the macula begins to deteriorate, the central vision that defines daily life starts to blur, distort, and fade. For millions of people worldwide, this is the lived reality of age-related macular degeneration.
AMD is the leading cause of severe central vision loss in people over 50 in high-income countries. The World Health Organization identifies it among the top causes of global visual impairment. Yet many people remain unaware of their risk, unaware of the warning signs, and unaware that effective treatments now exist — particularly for the most rapidly progressive form of the disease.
What Is Age-Related Macular Degeneration?
Age-related macular degeneration is a progressive eye condition that damages the macula — the central portion of the retina responsible for sharp, detailed central vision. The retina lines the back of the eye and converts light into electrical signals that the brain interprets as images. The macula handles the fine-detail work: reading, driving, threading a needle, and identifying faces all depend on it.
How the Macula Works
The macula contains the highest concentration of photoreceptor cells — specifically cone cells — in the entire retina. These cells require a rich and continuous supply of oxygen and nutrients, delivered via a layer of blood vessels called the choroid and supported by a single-cell layer called the retinal pigment epithelium, or RPE.
The RPE performs essential maintenance functions for the photoreceptors above it. It removes cellular waste products, recycles visual pigments, and regulates fluid balance. When the RPE begins to fail — as happens in AMD — photoreceptor cells gradually lose their support system and begin to deteriorate.
Why AMD Affects Central Vision
Because the macula occupies the central zone of the retina, AMD specifically affects central vision rather than peripheral vision. This means people with AMD can often still see around the edges of their visual field while losing the ability to see clearly in the centre. A dark, blurry, or distorted spot in the middle of vision — called a scotoma — is a hallmark of advanced AMD.
Peripheral vision generally remains intact in AMD, which is why the condition rarely causes total blindness. However, the loss of central vision dramatically restricts independence, making reading, driving, and many daily activities extremely difficult or impossible without appropriate support.
How Common Is AMD?
AMD affects an estimated 196 million people globally, with projections suggesting this number will exceed 288 million by 2040 as populations age worldwide. In the United States alone, the National Eye Institute estimates that over 11 million people have some form of AMD.
The Growing Burden of AMD
The prevalence of AMD rises steeply with age. Early AMD affects approximately 10% of people aged 60 to 69, rising to over 30% in those aged 80 and above. As global life expectancy increases and older populations grow, AMD is becoming one of the most significant public health challenges in eye care worldwide.
Despite its prevalence, AMD remains underdiagnosed. Many people attribute early visual changes to normal ageing and do not seek timely eye examination. This delay allows the condition to progress without intervention, increasing the risk of severe, irreversible vision loss.
The Two Main Types of AMD
AMD presents in two distinct forms — dry and wet — that differ substantially in their mechanisms, speed of progression, and treatment approaches. Understanding both types is essential for anyone seeking to manage or prevent the condition.
Dry AMD: The More Common Form
Dry AMD, also called atrophic AMD, accounts for approximately 80% to 90% of all AMD cases. It develops when the RPE and the photoreceptor cells it supports gradually break down over time. This breakdown occurs in part because of the accumulation of small yellowish deposits called drusen beneath the RPE.
Drusen are a hallmark feature of dry AMD. Small, hard drusen are common in normal ageing and carry limited risk. Larger, soft drusen — particularly when numerous — signal significantly elevated risk of AMD progression. As the condition advances, areas of RPE cell loss develop, causing patches of irreversible photoreceptor damage called geographic atrophy.
How Dry AMD Progresses
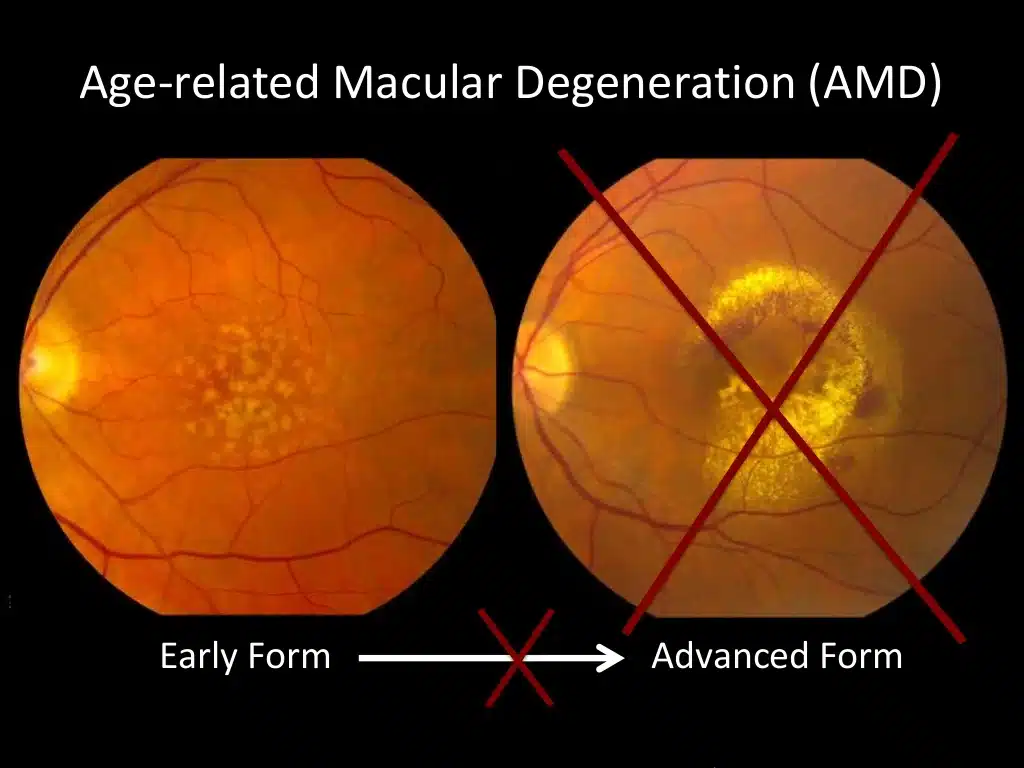
Dry AMD typically progresses slowly, often over many years. The condition passes through early, intermediate, and advanced stages. Early dry AMD involves small to medium drusen with no vision symptoms. Intermediate AMD involves larger drusen and sometimes mild central vision blurring or difficulty in low-light conditions.
Advanced dry AMD — geographic atrophy — involves significant RPE and photoreceptor cell loss producing a scotoma in central vision. Approximately 20% of people with advanced AMD have the dry geographic atrophy form rather than wet AMD, and until very recently no treatment existed to slow its progression.
Wet AMD: Less Common but More Aggressive
Wet AMD, also called neovascular or exudative AMD, accounts for approximately 10% to 15% of AMD cases but is responsible for the majority of severe, rapid central vision loss from the disease. Wet AMD develops when abnormal new blood vessels — a process called choroidal neovascularisation — grow beneath the retina from the choroid layer.
These new blood vessels are abnormal and fragile. They leak fluid and blood beneath and within the retinal layers, causing rapid distortion, swelling, and scarring of the macula. Unlike dry AMD, which progresses over years, wet AMD can cause significant central vision loss within weeks to months without treatment.
Warning Signs of Wet AMD Conversion
People with dry AMD face a risk of conversion to wet AMD at any time. Warning signs requiring urgent ophthalmological assessment include sudden onset of visual distortion — straight lines appearing wavy or bent — rapid central vision blurring, and a dark spot appearing or enlarging suddenly in central vision.
The Amsler grid, a simple self-monitoring tool using a grid of horizontal and vertical lines, helps people with AMD detect distortion between clinic appointments. Any sudden change detected on the Amsler grid warrants same-day contact with an eye care provider.
Risk Factors for AMD
AMD develops from an interaction of age, genetics, lifestyle, and environmental factors. Identifying personal risk factors helps people take targeted protective action.
Age and Genetic Risk
Age is the most significant risk factor for AMD. The condition is uncommon below age 50 and increases substantially in prevalence with each decade thereafter. Family history confers significant additional risk — people with a first-degree relative affected by AMD face two to four times the average risk.
Genetic research has identified several variants strongly associated with AMD risk. Variants in the complement factor H gene and the ARMS2 gene contribute meaningfully to AMD susceptibility. Genetic testing for AMD risk is available and may inform screening frequency decisions for high-risk individuals.
Lifestyle Risk Factors
Smoking is the single most powerful modifiable risk factor for AMD. Smokers face two to four times the risk of AMD compared to non-smokers, and the risk remains elevated for years after stopping. Every person concerned about AMD risk should understand that stopping smoking is the single most impactful protective action they can take.
Ultraviolet light exposure, poor diet low in antioxidants and leafy green vegetables, obesity, and cardiovascular disease all contribute to AMD risk. These factors share pathways involving oxidative stress and inflammation — both central mechanisms in AMD development — making cardiovascular and eye health deeply interconnected.
Blood Pressure, Cardiovascular Health, and AMD
Hypertension — high blood pressure — and cardiovascular disease associate with elevated AMD risk, particularly for wet AMD. The choroidal blood vessels that nourish the RPE and photoreceptors are vulnerable to the same vascular damage that affects cardiovascular health systemically.
Managing blood pressure through lifestyle and medication, maintaining healthy cholesterol levels, and addressing other cardiovascular risk factors benefits both heart health and long-term retinal health. This connection reinforces the systemic importance of lifestyle choices for preserving vision.
Diagnosing Age-Related Macular Degeneration
AMD diagnosis relies on detailed retinal examination and specialised imaging rather than standard vision testing alone.
Dilated Fundus Examination
A dilated fundus examination — in which eye drops widen the pupil to allow a direct view of the retina — enables the ophthalmologist to examine the macula, identify drusen, assess pigment changes, and detect any signs of fluid or bleeding indicating wet AMD. This examination forms the foundation of AMD assessment.
Routine vision testing alone does not detect early AMD reliably. People can have significant drusen accumulation without noticing any change in their visual acuity. This is why age-appropriate retinal examinations matter so much independently of vision complaint.
Optical Coherence Tomography in AMD
OCT has transformed AMD diagnosis and monitoring. This non-invasive imaging technique produces detailed cross-sectional images of the retinal layers, allowing clinicians to identify drusen, geographic atrophy, and — critically — the presence of fluid beneath or within the retina that signals wet AMD activity.
OCT-angiography, an advanced variant, visualises the blood vessels beneath the retina without requiring injection of a dye. This capability allows detection and monitoring of the abnormal vessel growth characteristic of wet AMD with exceptional detail and safety.
Fundus Fluorescein Angiography
Fluorescein angiography involves injecting a fluorescent dye into a vein in the arm and photographing its passage through the retinal blood vessels. This technique highlights abnormal vessel growth and leakage in wet AMD, helping clinicians define the extent and location of neovascularisation before and during treatment.
While OCT has reduced reliance on fluorescein angiography in routine monitoring, the technique remains valuable in certain diagnostic situations and in planning treatment for complex wet AMD presentations.
Treatment Options for Dry AMD
Until recently, no treatment existed to meaningfully slow the progression of dry AMD. The landscape has changed significantly in recent years, with new options now available for specific stages of the condition.
AREDS2 Nutritional Supplements
The Age-Related Eye Disease Study 2 — known as AREDS2 — produced the most influential evidence on nutritional supplementation in dry AMD. This large clinical trial demonstrated that a specific combination of vitamins and minerals significantly reduces the risk of progression from intermediate to advanced AMD.
The AREDS2 formula contains vitamin C, vitamin E, lutein, zeaxanthin, zinc, and copper. It reduces the risk of AMD progression by approximately 25% in people with intermediate AMD or advanced AMD in one eye. Importantly, the formula benefits people with intermediate or advanced disease — it does not prevent AMD in people with early disease or no AMD.
Complement Inhibitors for Geographic Atrophy
Geographic atrophy — advanced dry AMD — has historically had no approved treatment. Two complement inhibitors received regulatory approval in 2023 for reducing the rate of geographic atrophy growth. Pegcetacoplan, approved by the FDA, targets the complement protein C3. Avacincaptad pegol targets complement protein C5.
Both medications slow the growth of geographic atrophy lesions when administered as regular intravitreal injections — injections directly into the vitreous cavity of the eye. These treatments represent a landmark advance for a form of AMD that previously had no approved intervention, though vision improvement remains limited as existing photoreceptor loss cannot reverse.
Low Vision Rehabilitation
For people with advanced dry AMD causing significant visual impairment, low vision rehabilitation provides practical strategies and assistive technologies to maximise remaining vision. Magnifying devices, screen-reading software, high-contrast materials, and home modification advice all help maintain independence.
Low vision rehabilitation does not restore lost vision but significantly improves functional ability and quality of life. Referral to a low vision specialist should accompany any advanced AMD diagnosis.
Treatment Options for Wet AMD
Wet AMD treatment has undergone a revolution over the past two decades. Anti-VEGF therapy — the current standard of care — has transformed what was once a condition leading to rapid, inevitable severe vision loss into one that is manageable and in many cases improvable.
Anti-VEGF Injections: The Gold Standard
Anti-VEGF therapy targets vascular endothelial growth factor, the protein that drives the growth of abnormal blood vessels in wet AMD. By blocking VEGF, these medications stop abnormal vessel growth, reduce leakage, and allow the retina to dry out. In many people, vision improves significantly with treatment.
Several anti-VEGF agents are currently in widespread clinical use. Ranibizumab, bevacizumab, aflibercept, and brolucizumab all demonstrate efficacy in wet AMD clinical trials. Faricimab — the newest approved agent — blocks both VEGF and a complementary pathway, allowing longer intervals between injections in many people.
How Anti-VEGF Treatment Works
Anti-VEGF medications are administered as intravitreal injections — injections directly into the vitreous gel inside the eye. The procedure is performed in a clinical setting using local anaesthetic drops and takes only a few minutes. Most people describe mild discomfort or pressure rather than significant pain during the injection.
Treatment typically begins with a loading phase of monthly injections to achieve initial disease control. Maintenance injections then continue at intervals determined by monitoring results — either at fixed intervals or adjusted based on ongoing OCT imaging showing disease activity.
Treat-and-Extend and Pro Re Nata Protocols
Two main approaches govern the maintenance phase of anti-VEGF therapy. The treat-and-extend protocol involves progressively extending injection intervals when OCT shows no disease activity, aiming to reach the longest possible interval that maintains disease control. This approach reduces the treatment burden while maintaining vision gains.
The pro re nata — or as-needed — protocol involves monthly monitoring and injection only when OCT confirms disease activity. Both approaches aim to minimise injection burden while preserving the vision gains achieved during initial treatment. The optimal protocol varies between individuals and clinical settings.
Photodynamic Therapy
Photodynamic therapy, known as PDT, was the standard treatment for wet AMD before anti-VEGF therapy emerged. It involves injecting a light-sensitive drug called verteporfin intravenously, then activating it with a laser directed at the abnormal vessels in the eye. The activated drug selectively damages the abnormal vessels without harming surrounding tissue.
PDT is now used infrequently as a primary treatment for wet AMD, having been largely superseded by anti-VEGF therapy. However, it retains a role in combination treatment for certain subtypes of wet AMD — particularly polypoidal choroidal vasculopathy — where it performs better relative to anti-VEGF therapy alone.
Emerging Therapies and Gene Therapy
The treatment landscape for wet AMD continues to evolve rapidly. Gene therapy approaches aim to enable the eye itself to produce anti-VEGF proteins continuously, potentially eliminating the need for repeated injections. Early-phase clinical trials show promising results.
Port delivery systems — implantable devices that continuously release anti-VEGF medication inside the eye — are also under investigation and early clinical use. These innovations aim to address the significant burden of repeated clinic visits and injections that current wet AMD treatment demands.
Living with AMD: Protecting Vision Long Term
AMD is a lifelong condition requiring ongoing monitoring, lifestyle management, and — for wet AMD — sustained treatment engagement. Understanding what long-term management involves helps people approach the condition actively rather than passively.
Self-Monitoring at Home
The Amsler grid remains a valuable home monitoring tool for people with AMD, particularly those with dry AMD who are at risk of wet AMD conversion. Checking the grid daily with each eye separately and reporting any sudden change to an eye care provider ensures that wet AMD conversion receives the rapid treatment it requires.
Smartphone applications now offer digital versions of the Amsler grid and other visual monitoring tools. Several ophthalmology centres have developed remote monitoring systems that allow home-based detection of fluid changes requiring treatment, reducing the need for routine monitoring visits.
Diet and Lifestyle for AMD Protection
A diet rich in leafy green vegetables — particularly kale, spinach, and collard greens — provides lutein and zeaxanthin, carotenoids that concentrate in the macula and support its health. Oily fish, rich in omega-3 fatty acids, supports retinal vascular health. These dietary choices complement AREDS2 supplementation rather than replacing it.
Protecting eyes from ultraviolet light by wearing good-quality sunglasses outdoors reduces cumulative phototoxic damage to the retina. Maintaining a healthy weight, staying physically active, managing blood pressure, and — most importantly — not smoking all reduce AMD progression risk substantially.
Support Services and Adaptation
Living with AMD-related vision loss requires practical adaptation and emotional support. Organisations including the Macular Society, the American Macular Degeneration Foundation, and Fight for Sight provide educational resources, peer support communities, and practical guidance for people at all stages of the condition.
Emotional responses to AMD — including grief over lost visual abilities, anxiety about future progression, and frustration with treatment demands — are entirely normal and deserve acknowledgment alongside clinical management. Mental health support, peer connection, and low vision rehabilitation together help people maintain quality of life throughout their AMD journey.
Frequently Asked Questions
Can AMD be prevented?
AMD cannot be prevented entirely, given the significant role of age and genetics. However, modifiable risk factors offer genuine opportunities to reduce risk and slow progression. Stopping smoking, maintaining cardiovascular health, eating a diet rich in leafy vegetables and oily fish, protecting eyes from ultraviolet light, and taking AREDS2 supplements if recommended by an eye care provider all reduce AMD progression risk. Regular eye examinations from age 50 onwards enable early detection when intervention is most effective.
Does dry AMD always turn into wet AMD?
Not always, but the risk exists throughout life for anyone with dry AMD. Approximately 10% to 15% of people with dry AMD will develop wet AMD at some point, with risk increasing as dry AMD advances. People with intermediate or advanced dry AMD face higher conversion risk. This is why regular monitoring and home Amsler grid use are important — they enable rapid detection of conversion before significant vision loss occurs.
How quickly does wet AMD cause vision loss?
Wet AMD can cause significant central vision loss within weeks to months without treatment. This rapid progression distinguishes it from dry AMD, which typically progresses over years. Any sudden change in vision — new distortion, sudden blurring, or a dark spot appearing in central vision — requires same-day contact with an eye care provider. Prompt anti-VEGF treatment following wet AMD onset produces the best visual outcomes.
Are anti-VEGF injections painful?
Most people tolerate anti-VEGF injections well. Local anaesthetic eye drops numb the eye surface before the injection, and most people describe mild pressure or discomfort rather than significant pain during the procedure. Some people experience brief discomfort, floaters, or mild redness afterwards, which typically resolves within a day or two. The injection procedure takes only a few minutes and does not require general anaesthesia.
Can AMD affect both eyes?
Yes, AMD frequently affects both eyes, though often asymmetrically — one eye may be at a more advanced stage than the other. People with AMD in one eye face significantly elevated risk of developing the condition in the fellow eye. This bilateral risk makes comprehensive monitoring of both eyes essential and underscores the importance of treatment that considers long-term disease management in both eyes simultaneously.
Is AMD hereditary?
AMD has a significant genetic component. People with one or more first-degree relatives diagnosed with AMD face two to four times the average risk of developing the condition. Identified genetic variants in the complement pathway and other genes contribute meaningfully to AMD susceptibility. However, genetics does not determine destiny — lifestyle factors, particularly smoking cessation and diet, substantially modify genetic risk and influence whether and when AMD develops.
Conclusion
Age-related macular degeneration steals central vision gradually in dry AMD and rapidly in wet AMD — but the story does not end there. Treatment has transformed the outlook for both forms of this condition in recent decades. AREDS2 supplements slow dry AMD progression. Anti-VEGF therapy preserves and often improves vision in wet AMD. New complement inhibitors address geographic atrophy. Gene therapy and port delivery systems promise to reduce treatment burden further in coming years.
The most critical factor in every case remains the same: early detection. Regular retinal examinations from age 50 onwards, self-monitoring with the Amsler grid, and prompt reporting of any visual change give treatment every opportunity to protect the central vision that AMD threatens. Lifestyle choices — particularly stopping smoking — add further protection that no medication can replicate.
AMD does not have to mean the end of independent, visually engaged life. With appropriate treatment, monitoring, and support, most people with AMD retain meaningful vision for many years. The key is knowing the risk, attending regular check-ups, and acting quickly when vision changes.
References
- The research reveals that money plays a much bigger role in dating than many people realize.
- OpenAI’s agreement with AMD includes a commitment to refine AMD’s line of Instinct GPUs, which are positioned as competitors to Nvidia’s products.
- The RBI’s latest steps are part of a broader strategy to stabilize borrowing costs and support economic growth.
Disclaimer:
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis, treatment, or any eye health concerns.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.