
Acute Lymphoblastic Leukemia (ALL) in Adults: How It Differs From the Childhood Type
When 42-year-old Jennifer developed persistent fatigue, bruising, and bone pain, blood tests revealed acute lymphoblastic leukemia—the same cancer most common in young children. Her oncologist delivered sobering news: while children with ALL have cure rates exceeding 90%, adults like Jennifer face a much tougher battle. “I couldn’t understand it,” Jennifer recalled. “How could the exact same disease be so much deadlier in adults? It didn’t make sense.” Her confusion reflects a medical paradox that has puzzled researchers for decades.
Children diagnosed with acute lymphoblastic leukemia have an excellent prognosis, with cure rates exceeding 85%. However, the prognosis for ALL declines with increasing age, with historic cure rates of just 30% to 40% in adults. The significant drop from ages 17 to 20 years accounts for 45% of the total survival decrease between the ages of 17 to 70 years and is known as the “survival cliff” PubMed Central. This dramatic survival cliff represents one of oncology’s most striking age-related disparities. Understanding why the same cancer behaves so differently across age groups reveals important lessons about disease biology, treatment tolerance, and the complex interplay between cancer and aging.
The Survival Gap: Numbers That Tell A Stark Story
The overall five-year survival rate for ALL is 72%. Young children have the highest survival rate, around 90%. The five-year survival rate for adults with ALL is around 30% to 40% Cleveland Clinic. Breaking this down further shows how survival declines steadily with age. Children under 15 achieve approximately 90% cure rates with modern treatment. Adolescents aged 15-19 see this drop to around 70-75%. Young adults in their twenties experience 50-60% five-year survival. By ages 40-59, survival falls to 28-43%. Adults over 60 face particularly grim odds, with five-year survival rates below 20%, and those over 70 seeing survival rates around 6%.
The overall 5-year survival rates have improved significantly over time, from 51% before 1990 to 72% since 2010. The survival rates for children aged 0 to 14 years and adolescents aged 15 to 19 years have improved from 73% and 55% before 1990 to 93% and 74% since 2010, respectively. The rates remained under 30% in older patients (60+ years) PubMed Central. While all age groups have seen improvements over recent decades, the gap between children and adults persists stubbornly. The question is: why?
Different Biology: Not The Same Disease After All
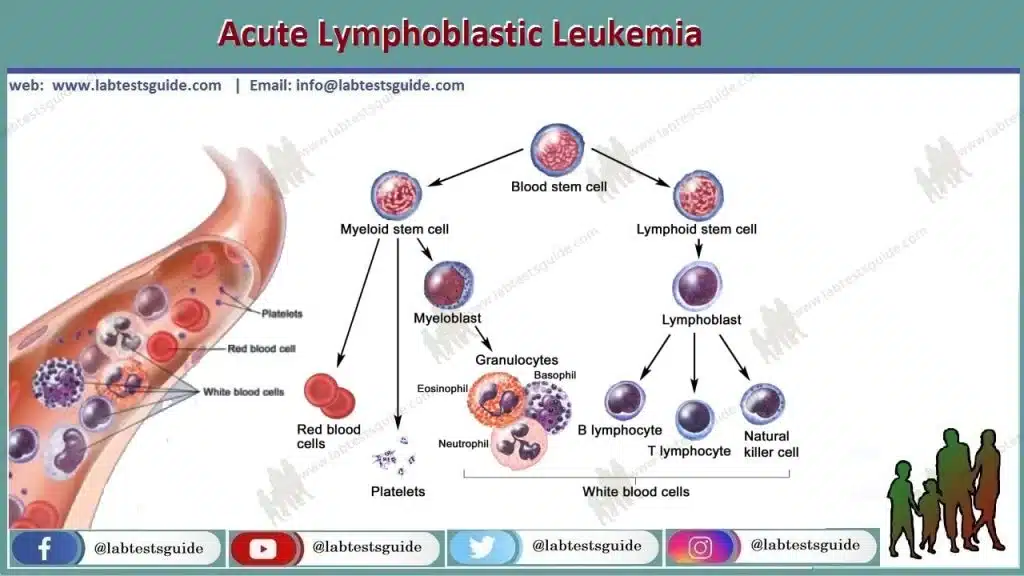
The first major difference lies in the genetic makeup of ALL itself. ALL isn’t a single uniform disease—it’s actually many different subtypes defined by specific chromosomal abnormalities and gene mutations. These subtypes occur at vastly different frequencies in children versus adults, fundamentally changing disease biology and treatment response.
A major contributing factor that influences prognosis in this population is the reduced prevalence of genetic subtypes associated with favorable outcome and a concomitant increase in subtypes associated with poor outcome PubMed Central. Children with ALL frequently harbor favorable genetic changes like ETV6-RUNX1 fusion (occurring in about 25% of childhood cases) and high hyperdiploidy (extra chromosomes, seen in 25-30% of children). These subtypes respond excellently to standard chemotherapy, driving the high cure rates in pediatric ALL.
Adults, conversely, rarely develop these favorable subtypes. Instead, adults show much higher rates of poor-prognosis genetic abnormalities. The Philadelphia chromosome (BCR-ABL1 fusion) occurs in only 3-5% of childhood ALL but affects 25-30% of adult cases—and until recently, predicted dismal outcomes. Other high-risk genetic features like complex karyotype, low hypodiploidy, and certain mixed-lineage leukemia rearrangements also increase with age. Even when adults develop the same genetic subtype as children, it often behaves more aggressively, suggesting that age itself modifies cancer biology in ways we don’t fully understand.
Treatment Tolerance: The Body’s Declining Resilience
Current treatment relies on multiagent chemotherapy administered over 2–3 years, resulting in long-term survival in 80–90% in pediatric patients compared to 40%–50% in adult patients, depending upon patient- and disease-specific characteristics PubMed Central. ALL treatment requires intensive, prolonged chemotherapy lasting 2-3 years, divided into induction (initial attack on leukemia), consolidation (eliminating remaining cells), and maintenance (long-term low-dose therapy preventing relapse). This regimen includes multiple toxic drugs—vincristine, steroids, asparaginase, anthracyclines, methotrexate—each with serious side effects.
Children tolerate this brutal treatment remarkably well. Their young organs—liver, kidneys, heart—repair damage more efficiently. They recover faster from chemotherapy-induced low blood counts. Infectious complications, while serious, typically resolve with antibiotics. Children can receive higher chemotherapy doses relative to body weight without experiencing the severe complications that plague adults.
Adults struggle profoundly with the same treatment protocols. Older livers metabolize drugs less efficiently, leading to higher toxicity. Hearts damaged by years of hypertension or previous medical conditions cannot withstand anthracycline chemotherapy that children tolerate easily. Kidney function declines naturally with age, making high-dose methotrexate dangerous. Infections prove more severe and harder to clear. Many adults cannot complete the full intended treatment due to life-threatening complications, resulting in suboptimal therapy and higher relapse rates.
Steroid-induced side effects particularly devastate adults. While children may experience mood changes and weight gain, adults develop severe diabetes, psychosis, muscle wasting, bone death (avascular necrosis), and opportunistic infections that can prove fatal. The very treatments that cure children often harm adults before they can eliminate the leukemia.
Treatment Differences: Protocol Matters
For decades, children and adults received entirely different ALL treatment protocols. Pediatric oncologists developed regimens through Children’s Oncology Group trials, emphasizing intensive multi-drug therapy with prolonged maintenance. Adult oncologists used less intensive approaches, fearing toxicity in older patients. This created a self-fulfilling prophecy: adults received gentler treatment, experienced higher relapse rates, and confirmed the belief that adult ALL was incurable.
It is a new and exciting time for acute lymphoblastic leukemia. While nearly 50 years ago, only one in nine children with ALL survived with chemotherapy, nowadays nearly 90% of children have a chance of long-term survival. Adults with ALL, as well as the special category of adolescents and young adult patients, are catching up with the new developments seen in children, but still their prognosis is much worse PubMed Central.
A breakthrough came when researchers noticed that adolescents and young adults treated on pediatric protocols fared significantly better than similar-age patients treated on adult protocols. The outcome of adolescents and young adults with ALL has improved significantly in the last decade due to the increased use of pediatric-inspired regimens. Event-free survival and overall survival rates of 66% and 79% were achieved when patients ages 17 to 39 years were treated with pediatric-inspired protocols PubMed Central. This observation sparked a revolution: treating younger adults with pediatric-style intensive therapy dramatically improved outcomes, proving that treatment approach—not just age—drives results.
Now, many centers treat adults up to age 40 or even 60 with modified pediatric regimens, balancing intensity against toxicity. Survival rates for young adults have improved substantially, narrowing (though not eliminating) the gap with children.
The Philadelphia Chromosome Success Story
One bright spot in adult ALL involves Philadelphia chromosome-positive disease. Historically considered a poor risk ALL subtype, the treatment and outcome of Philadelphia chromosome-positive B-cell ALL were drastically changed with the advent of the BCR-ABL1 tyrosine kinase inhibitors. The combination of a TKI with a backbone of multiagent chemotherapy, or more recently blinatumomab, is the mainstay of therapy, resulting in 5-year survival rates of 80+% PubMed Central.
Before 2001, Philadelphia chromosome-positive ALL was essentially a death sentence, with cure rates under 10%. The introduction of imatinib (Gleevec) and newer tyrosine kinase inhibitors like dasatinib and ponatinib transformed outcomes. Adding these targeted drugs to chemotherapy yields cure rates exceeding 80%—better than many other ALL subtypes. This proves that when we understand specific molecular drivers and target them effectively, age matters less.
Other Biological Differences
Beyond genetics and treatment tolerance, several other factors contribute to worse adult outcomes. Minimal residual disease—microscopic leukemia remaining after treatment—clears more slowly in adults, indicating resistant disease. Adults show higher rates of treatment-resistant disease from the start, with more patients failing to achieve initial remission. Central nervous system involvement, where leukemia cells hide in the brain and spinal fluid, occurs more frequently in adults and proves harder to eradicate.
The immune system’s role also differs. Children’s robust immune systems may help eliminate residual leukemia cells after chemotherapy reduces the cancer burden. Adults’ aging immune systems, already weakened by decades of exposure to infections and natural immune senescence, contribute less effectively to leukemia eradication.
Socioeconomic And Access Factors
Beyond biology, practical factors worsen adult outcomes. Children typically receive treatment at specialized pediatric cancer centers with extensive support services—dedicated nurses, child life specialists, nutritionists, and social workers ensuring treatment completion. Adults often receive care at community hospitals with less ALL expertise. Clinical trial participation—providing access to cutting-edge treatments—is standard for children but much lower for adults.
Financial toxicity hits adults harder. Children on parents’ insurance face fewer out-of-pocket costs than adults responsible for copays, deductibles, and lost income during prolonged treatment. Many adults delay or abandon treatment due to financial concerns—unthinkable for children whose families mobilize all resources for cure.
Frequently Asked Questions
Q1: I’m an adult just diagnosed with ALL. Does this mean I can’t be cured?
No—cure is definitely possible, though more challenging than in children. Your specific subtype, genetic features, and response to initial treatment matter enormously. Philadelphia chromosome-positive ALL, once deadly, now achieves 80%+ cure rates with targeted therapy. If you’re under 40 and relatively healthy, treatment with pediatric-inspired intensive protocols can achieve 60-70% long-term survival. Even older adults can achieve remission and prolonged survival with appropriate therapy. Your oncologist will assess your individual risk factors—genetic abnormalities, white blood cell count, how quickly you respond to treatment—to provide personalized prognosis. Many adults are cured; it just requires more intensive treatment and closer monitoring than in children.
Q2: Why can’t I just take the same treatment that cures 90% of children?
You essentially will receive similar treatment, but your body tolerates it differently. The same chemotherapy drugs that children handle relatively well cause more severe complications in adults. Your liver, kidneys, and heart don’t bounce back from toxic chemotherapy as quickly as a child’s. You’re more likely to develop life-threatening infections, organ damage, or severe side effects requiring dose reductions. Many adult treatment protocols are actually modified pediatric regimens, adjusted for adult physiology. Some adults under 40 at specialized centers receive nearly identical treatment to children, accepting higher toxicity for better cure rates. The challenge isn’t giving you pediatric treatment—it’s getting you through it safely.
Q3: Are there any advantages adults have in ALL treatment?
Adults have some benefits children lack: better ability to communicate symptoms early, allowing prompt intervention for complications; capacity to understand and participate in treatment decisions, improving adherence; adult bodies that can tolerate certain targeted therapies being developed specifically for adult ALL subtypes; and eligibility for clinical trials testing novel drugs that may work better with less toxicity than traditional chemotherapy. Additionally, your mature immune system, while weaker than a child’s, may respond better to immunotherapy approaches like CAR-T cell therapy and blinatumomab—treatments revolutionizing adult ALL management.
Q4: What’s the “survival cliff” between ages 17-20, and why does it happen?
The survival cliff describes the dramatic survival drop from late teenage years (70-75% five-year survival) to early twenties (50-60% survival) to thirties (40-50% survival). This sharp decline happens because: genetic subtypes shift rapidly—favorable subtypes common in children virtually disappear by the twenties while poor-prognosis subtypes increase; treatment transitions occur—adolescents often receive pediatric treatment while young adults get adult protocols, creating outcome gaps; and physiological changes related to completing puberty may affect how leukemia behaves and responds to treatment. The cliff isn’t a single age cutoff but rather reflects this transition period where childhood-favorable biology gives way to adult-unfavorable patterns.
Q5: Is ALL treatment improving for adults like it has for children?
Yes, though progress is slower. Since 2010, adult ALL survival has improved from 24-33% to 43-59% for ages 40-59—still far behind children but significantly better than historical rates. Improvements come from: adopting pediatric-inspired treatment protocols for younger adults; adding targeted therapies like tyrosine kinase inhibitors for Philadelphia chromosome-positive disease; using immunotherapy drugs like blinatumomab and CAR-T cells that work particularly well in adults; better supportive care preventing treatment complications; and improved minimal residual disease monitoring allowing treatment adjustments. Research continues developing less toxic but equally effective treatments specifically designed for adult ALL biology.
Disclaimer
This article adapts publicly available information from reputable medical research organizations and cancer databases. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform — not a healthcare provider. Decisions about acute lymphoblastic leukemia diagnosis and treatment should be made in consultation with qualified hematologists and oncologists who can evaluate your individual disease characteristics, genetic profile, treatment tolerance, and overall health. If you have been diagnosed with ALL, please consult with your healthcare team promptly to discuss appropriate treatment options tailored to your age and specific disease features.
References
- PMC. Genetics and prognosis of ALL in children vs adults. https://pmc.ncbi.nlm.nih.gov/articles/PMC6245970/
- Cleveland Clinic. Acute Lymphoblastic Leukemia (ALL). https://my.clevelandclinic.org/health/diseases/21564-acute-lymphocytic-leukemia
- PMC. Adult Acute Lymphoblastic Leukemia: 2025 Update on Diagnosis, Therapy, and Monitoring. https://pmc.ncbi.nlm.nih.gov/articles/PMC12712861/
- PMC. Why Do Children with Acute Lymphoblastic Leukemia Fare Better Than Adults? https://pmc.ncbi.nlm.nih.gov/articles/PMC8345615/
- PMC. Acute lymphoblastic leukemia: A population-based study of outcome in the United States based on the SEER database. https://pmc.ncbi.nlm.nih.gov/articles/PMC9517941/
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.