
Ebola virus disease: The deadly hemorrhagic fever we’re learning to fight with vaccines and monoclonal antibodies
Ebola virus disease: 50% fatality rate—vaccines, treatments now available
Dr. Fatoumata Koroma will never forget the day Ebola arrived at her clinic in rural Guinea.
It was March 2014. A young man stumbled through the door with high fever, severe headache, and muscle pain. Within hours, he began vomiting violently. By the next morning, he was bleeding from his gums and eyes.
“We didn’t know what we were dealing with,” Fatoumata recalled. “We’d heard rumors about a strange illness in villages to the north, but nothing prepared us for what we saw. Within days, three nurses who’d cared for him developed the same symptoms. Within two weeks, all four were dead.”
What started in that small clinic became the largest Ebola virus disease outbreak in history—the 2014-2016 West Africa outbreak that killed more than 11,000 people across Guinea, Sierra Leone, and Liberia. More deaths than all previous Ebola outbreaks combined.
But here’s what’s changed since then: we now have vaccines that can protect people before exposure and monoclonal antibody treatments that dramatically improve survival for those infected. The disease that once seemed unstoppable is becoming controllable—if we act fast enough.
Understanding the Killer
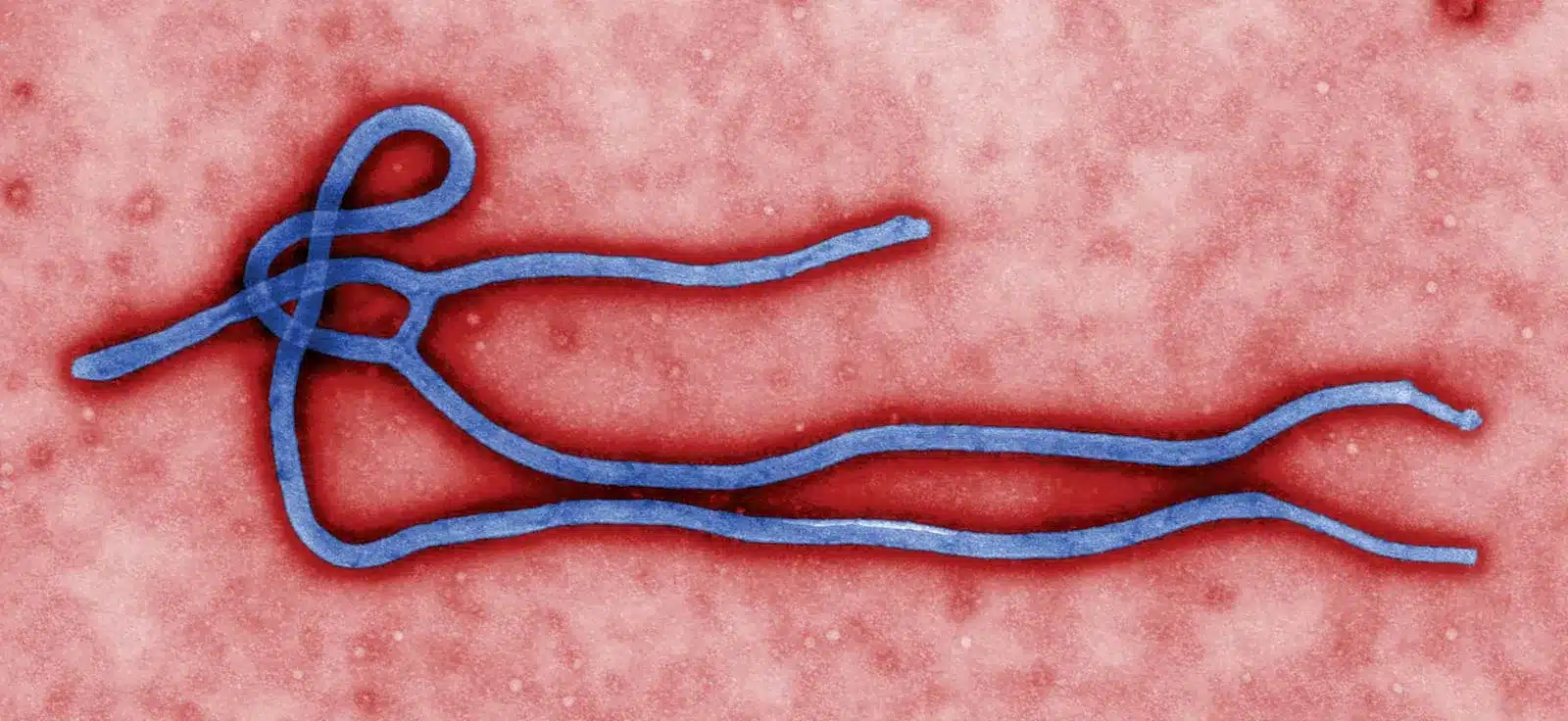
Ebola virus disease is a severe, often fatal illness affecting humans and other primates. The virus belongs to a family called filoviruses, which cause hemorrhagic fevers—diseases that damage blood vessels and impair the body’s ability to clot.
According to WHO fact sheets on Ebola disease, the average case fatality rate is around 50%. In past outbreaks, this rate has varied from 25% to 90%, depending on which strain of the virus was involved and the quality of medical care available.
The first Ebola outbreaks occurred in 1976 in remote villages in Central Africa near tropical rainforests—hence the name, taken from the Ebola River in what is now the Democratic Republic of the Congo.
Scientists believe fruit bats of the Pteropodidae family are natural hosts of the virus. These bats carry the virus without getting sick themselves, but can transmit it to other animals and humans.
How Ebola Spreads—and Doesn’t
The virus is transmitted to people from wild animals such as fruit bats, porcupines, and non-human primates through contact with blood, organs, or other bodily fluids. This often happens when people hunt, butcher, or eat infected animals.
Once the virus jumps to humans, it spreads through direct contact with the blood, secretions, organs, or other bodily fluids of infected people, and with surfaces and materials like bedding or clothing contaminated with these fluids.
Here’s a critical detail: the incubation period—the time from infection to symptom onset—ranges from 2 to 21 days. During this time, an infected person cannot spread the disease. You can’t catch Ebola from someone who has the virus but doesn’t yet have symptoms.
This is vastly different from diseases like COVID-19 or influenza. Ebola doesn’t spread through the air. You can’t catch it by being in the same room as someone who’s infected. You have to have direct contact with bodily fluids.
But this also means healthcare workers, family members caring for the sick, and people preparing bodies for burial face extremely high risk. In past outbreaks, healthcare workers represented a disproportionate number of cases because they had the most contact with infected bodily fluids.
For more on outbreak prevention, see our article on infection prevention and control in healthcare settings.
When Symptoms Strike
Symptoms can be sudden and include fever, fatigue, malaise, muscle pain, headache, and sore throat. These initial symptoms are non-specific—they could be malaria, typhoid fever, meningitis, or dozens of other diseases.
But then the disease progresses. Vomiting, diarrhea, and abdominal pain follow. A rash may appear. Kidney and liver functions become impaired. In some cases—the images that haunt people’s nightmares—internal and external bleeding occurs. Patients may ooze blood from their gums or pass blood in their stools.
“The bleeding isn’t as common as people think from movies,” explained Dr. James Omondi, an infectious disease specialist who worked during the West Africa outbreak. “Most patients die from organ failure and shock, not hemorrhage. But the bleeding cases are the ones that stick in your memory forever.”
It can be difficult to clinically distinguish Ebola from other infectious diseases, so laboratory confirmation is essential. Diagnostic tests detect the virus’s genetic material or proteins in blood samples.
The 2014-2016 Crisis
The West Africa outbreak marked a turning point in Ebola’s history.
Previous outbreaks had occurred in remote villages in Central Africa. They burned out quickly because the villages were isolated, and the virus killed so efficiently that it couldn’t spread far before running out of hosts.
But the 2014-2016 outbreak started in Guinea and spread across land borders to Sierra Leone and Liberia. These countries had weak health systems, ongoing conflicts, high population mobility, and dense urban areas where the virus could spread far more effectively than in isolated villages.
There were more cases and deaths in this outbreak than all previous Ebola outbreaks combined. International health systems struggled to respond. Healthcare workers died by the hundreds. Entire communities were devastated.
Fatoumata, the doctor whose clinic was one of the first affected, contracted Ebola herself while caring for patients. “I thought I would die,” she said. “The fever was unbearable, the pain excruciating. I kept thinking about my three children, wondering who would care for them.”
She survived—barely. Many of her colleagues didn’t.
Breakthrough Treatments
The good news: we now have treatments that work.
For Ebola virus disease, WHO recommends treatment with monoclonal antibodies: mAb114 (ansuvimab™) or REGN-EB3 (Inmazeb™). These laboratory-made antibodies attach to the Ebola virus and help the immune system destroy it.
Clinical trials conducted during outbreaks showed these treatments dramatically improve survival rates when given early in the disease course. Patients receiving monoclonal antibodies within days of symptom onset had survival rates above 90%—a complete reversal from the historical 50% fatality rate.
Early intensive supportive care—rehydration with oral or intravenous fluids and treatment of specific symptoms—also improves survival substantially.
WHO has developed a CORE trial protocol for Filovirus treatments to rapidly evaluate new therapies during outbreaks.
Game-Changing Vaccines
Perhaps even more important than treatments are vaccines that prevent infection in the first place.
Two vaccines have been approved for Ebola virus disease: Ervebo® and the two-dose combination of Zabdeno® and Mvabea®. WHO recommends Ervebo vaccine as part of outbreak response.
The vaccines work through “ring vaccination”—a strategy where you vaccinate everyone who had contact with a confirmed case, plus contacts of those contacts. This creates a protective ring around each case, preventing further spread.
Ring vaccination proved remarkably effective during recent outbreaks in the Democratic Republic of the Congo. In a groundbreaking vaccination trial launched in Uganda in February 2025, researchers are studying how to optimize vaccine deployment.
Several candidate vaccines are at different stages of development for other Ebola species (there are six known species of Ebola virus).
Current Threat
Ebola hasn’t disappeared. Multiple outbreaks have occurred in recent years:
- Democratic Republic of the Congo, September 2025
- Uganda, 2022
- DRC Équateur Province, 2022
- DRC North Kivu, 2021
- Guinea, 2021
WHO maintains disease outbreak news with updates on active outbreaks and provides online training to strengthen Filovirus outbreak response, launched in March 2025.
Community Engagement: The Secret Weapon
Here’s something movies about Ebola never show: community engagement is absolutely essential to controlling outbreaks.
Outbreak control relies on clinical care, surveillance and contact tracing, laboratory services, infection prevention and control in health facilities, safe and dignified burials, vaccination, and social mobilization.
But all of these require community trust and participation.
During the West Africa outbreak, burial practices became a major transmission route. Traditional funerals involved washing and touching the body—and Ebola virus remains in bodily fluids after death. Communities had to change practices that had cultural and religious significance.
WHO’s Risk communication and community engagement readiness and response toolkit for Ebola, published in July 2025, provides practical tools for engaging communities.
“You can’t come into a community as an outsider and demand people change how they bury their loved ones,” explained Mariama Kamara, a community health worker in Liberia. “You have to listen, understand their beliefs, work with traditional leaders, and find solutions that honor both safety and dignity.”
The Framework and toolkit for infection prevention and control outbreak preparedness, published December 2025, emphasizes health facility readiness.
What Must Happen
To prevent future catastrophic outbreaks, several actions are essential:
Strengthen health systems in countries where Ebola is endemic. Strong primary healthcare, laboratory capacity, and infection prevention measures can detect and contain outbreaks early.
Maintain vaccine stockpiles through the International Coordinating Group on Vaccine Provision so doses are available immediately when outbreaks occur.
Invest in research to develop better diagnostics, treatments, and vaccines. WHO’s R&D Blueprint for Ebolavirus coordinates global research efforts.
Support survivors. Ebola survivors face ongoing health challenges and often severe stigma. WHO provides psychological first aid guidance for outbreak settings.
Improve surveillance to detect outbreaks early when they’re still small and containable. WHO’s work on rapidly detecting and responding to health emergencies is critical.
Train healthcare workers in proper infection prevention and control. WHO offers learning resources on Ebola diseases through its OpenWHO platform.
Fatoumata, who survived Ebola infection, now trains healthcare workers across West Africa in infection prevention. “I show them my scars,” she said. “I tell them what happened to my colleagues who didn’t follow protocols. And I tell them about the tools we have now—vaccines, treatments—that didn’t exist then. We can’t prevent every outbreak, but we can prevent every outbreak from becoming an epidemic.”
With vaccines that work, treatments that save lives, and growing understanding of how to engage communities, Ebola virus disease is becoming a controllable threat. But only if we maintain vigilance, invest in preparedness, and act decisively when outbreaks occur.
Frequently Asked Questions (FAQs)
Ebola virus disease is a severe, often fatal illness affecting humans and other primates, caused by filoviruses that damage blood vessels and impair clotting. According to WHO, the average case fatality rate is around 50%, though this has varied from 25-90% in past outbreaks depending on virus strain and quality of medical care. The virus was first discovered in 1976 in Central Africa near tropical rainforests. The largest outbreak occurred in West Africa during 2014-2016, killing over 11,000 people in Guinea, Sierra Leone, and Liberia—more deaths than all previous outbreaks combined. Fruit bats of the Pteropodidae family are believed to be natural hosts. The virus spreads to people from wild animals (fruit bats, porcupines, non-human primates) through contact with blood or bodily fluids, then spreads between humans through direct contact with infected fluids or contaminated surfaces. See WHO Q&A on Ebola for details.
The incubation period ranges from 2-21 days; infected people cannot spread the disease until symptoms develop. According to WHO fact sheets, symptoms can be sudden and include fever, fatigue, malaise, muscle pain, headache, and sore throat, followed by vomiting, diarrhea, abdominal pain, and rash. Later stages show impaired kidney and liver functions. In some cases, internal and external bleeding occurs (oozing from gums, blood in stools), though this is less common than portrayed in media. It’s difficult to clinically distinguish Ebola from other infectious diseases like malaria, typhoid fever, and meningitis, so laboratory confirmation is essential. Diagnostic tests detect the virus’s genetic material or proteins in blood samples. Healthcare workers, family caregivers, and those preparing bodies for burial face highest risk due to direct contact with bodily fluids. Unlike COVID-19 or influenza, Ebola doesn’t spread through air—you cannot catch it by being in the same room as an infected person without direct bodily fluid contact.
Treatment has advanced significantly in recent years. For Ebola virus disease, WHO recommends monoclonal antibody treatments: mAb114 (ansuvimab™) or REGN-EB3 (Inmazeb™). Clinical trials showed these laboratory-made antibodies dramatically improve survival—patients receiving treatment within days of symptom onset had survival rates above 90%, reversing the historical 50% fatality rate. Early intensive supportive care including rehydration with oral or intravenous fluids and treatment of specific symptoms also improves survival substantially. For other Ebola virus species, there are no approved therapeutics yet, but candidate products are under development. WHO has developed a CORE trial protocol to rapidly evaluate new therapies during outbreaks. WHO also published therapeutic prioritization for Marburg virus (another filovirus) in January 2025 and provides clinical management guidance.
Yes, two vaccines have been approved for Ebola virus disease: Ervebo® and the two-dose combination of Zabdeno® and Mvabea®. According to WHO guidance on Ebola vaccines, the Ervebo vaccine is recommended as part of outbreak response. Vaccines work through “ring vaccination”—vaccinating everyone who had contact with a confirmed case plus their contacts, creating a protective ring around each case to prevent further spread. This strategy proved remarkably effective during recent DRC outbreaks. A groundbreaking vaccination trial launched in Uganda in February 2025 studies optimal deployment strategies. Several candidate vaccines for other Ebola species are at various development stages. WHO coordinates vaccine stockpiles through the International Coordinating Group on Vaccine Provision ensuring doses are available immediately when outbreaks occur. WHO also maintains vaccine standardization activities.
Outbreak control requires multiple coordinated interventions. According to WHO, community engagement is key to successfully controlling any outbreak—communities must trust health authorities and participate in response measures. Control relies on clinical care, surveillance and contact tracing, laboratory services, infection prevention and control in health facilities, safe and dignified burials, vaccination (when available), and social mobilization. WHO’s Risk communication and community engagement toolkit (July 2025) and Framework for infection prevention and control outbreak preparedness (December 2025) provide practical guidance. Prevention requires strengthening health systems in endemic countries, maintaining vaccine stockpiles, investing in research through WHO’s R&D Blueprint, training healthcare workers via OpenWHO learning resources, improving surveillance to detect outbreaks early, and supporting survivors who face ongoing health challenges and stigma with psychological first aid. WHO launched online training to strengthen Filovirus outbreak response in March 2025.
- WHO Ebola Virus Disease Health Topic
- WHO Ebola Disease Fact Sheet
- WHO Ebola Q&A
- WHO Ebola Vaccines Q&A
- West Africa Outbreak 2014-2016
- DRC Ebola Outbreak 2025 Appeal
Disclaimer: This article is an adaptation of publicly available information from WHO’s Ebola virus disease
health topic page (WHO, Geneva. Licence: CC BYNC-SA 3.0 IGO). WHO is not responsible for the
content or accuracy of this adaptation. This content is for informational and educational purposes
only and does not constitute medical advice. ObserverVoice.com is a news and information platform
— not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.