
Hidradenitis Suppurativa: The Painful Skin Condition That Is Often Misdiagnosed for Years
Some skin conditions are immediately visible and easily recognised. Hidradenitis suppurativa is not among them, and that invisibility causes enormous suffering.
This chronic inflammatory condition causes painful, recurring lumps deep beneath the skin surface. These lumps form in areas where skin rubs together, such as the armpits, groin, buttocks, and under the breasts.
Hidradenitis suppurativa, commonly abbreviated as HS, affects approximately 1% of the global population. Despite this prevalence, most patients wait seven to ten years before receiving an accurate diagnosis, enduring unnecessary pain and emotional distress throughout that time.
What Is Hidradenitis Suppurativa?
Hidradenitis suppurativa is a chronic, debilitating inflammatory skin disease affecting hair follicles in areas where skin surfaces contact each other. It does not involve sweat glands directly, despite what the name historically suggested.
The condition causes repeated episodes of painful nodules, abscesses, and eventually scarring tunnels beneath the skin. These tunnels, called sinus tracts, connect multiple lesions and are a hallmark feature of more advanced disease.
Why HS Is Frequently Misdiagnosed
Most people with HS first receive a misdiagnosis of boils, folliculitis, ingrown hairs, or recurrent skin infections. General practitioners without specialist dermatology training may not immediately recognise the characteristic pattern of recurring lesions in specific anatomical locations.
The resulting diagnostic delay means many patients receive repeated antibiotic courses for presumed infections without addressing the underlying inflammatory disease process. This delay allows progressive skin damage, scarring, and psychological harm to accumulate over years or decades.
How HS Differs From Ordinary Boils
Ordinary boils arise from bacterial infection of a single hair follicle and resolve fully with treatment. HS lesions recur repeatedly in the same locations, do not consistently respond to antibiotics, and progressively worsen over time without proper management.
The presence of multiple recurrent lesions in characteristic locations, combined with tunnel formation and scarring, clearly distinguishes HS from simple boils. Recognising this clinical pattern is the essential first step toward correct diagnosis and effective treatment.
Understanding the Causes of Hidradenitis Suppurativa
The precise cause of hidradenitis suppurativa involves multiple interacting factors rather than a single definitive trigger. Researchers now understand it as a disease of follicular occlusion combined with dysregulated immune inflammation.
The process begins when a hair follicle becomes blocked by keratin, the structural protein making up skin and hair. This blockage causes the follicle to rupture, releasing its contents into the surrounding tissue and triggering intense inflammatory responses.
Genetic Factors in HS Development
Genetics play a significant role in hidradenitis suppurativa development. Approximately one-third of affected individuals report a first-degree relative with the same condition, suggesting a strong hereditary component.
Mutations in genes encoding components of the gamma-secretase complex, which regulates hair follicle development and immune signalling, have been identified in some familial HS cases. These genetic variants predispose individuals to follicular occlusion and exaggerated inflammatory responses in affected skin areas.
Immune System Dysregulation
HS involves overactivation of specific immune pathways, particularly those driven by tumour necrosis factor-alpha (TNF-α) and interleukins including IL-1β, IL-17, and IL-23. These inflammatory proteins drive the painful, destructive tissue response that characterises active HS lesions.
This immune dysregulation explains why HS responds to biological therapies targeting these specific pathways. Understanding the immunological basis of HS has fundamentally transformed how specialists approach treatment for moderate to severe disease.
Hormonal Influences on HS
Hormonal factors significantly influence HS activity, particularly in relation to androgens. Many people with HS notice worsening around menstrual periods, and the condition predominantly emerges after puberty when androgen levels rise.
Androgen hormones stimulate sebaceous gland activity and alter follicular keratinisation, contributing to follicular blockage. This hormonal link explains why anti-androgenic medications reduce disease activity in some affected individuals.
Recognised Risk Factors for Hidradenitis Suppurativa
Several factors increase the risk of developing HS or worsening existing disease. Understanding these risk factors helps both patients and clinicians make informed decisions about lifestyle modifications alongside medical treatment.
Obesity is among the most well-documented risk factors for HS. Excess body weight increases skin friction in affected areas, promotes a pro-inflammatory metabolic state, and raises androgen levels, all of which contribute to disease development and progression.
Smoking and HS Severity
Smoking is strongly associated with both increased HS risk and greater disease severity. Research consistently shows that smokers with HS experience more extensive disease, more frequent flares, and poorer responses to treatment than non-smokers.
The mechanisms involve nicotine’s effects on follicular keratinisation, skin immune responses, and wound healing capacity. Smoking cessation forms a genuinely important component of HS management, though it rarely eliminates disease activity on its own.
Other Contributing Risk Factors
Mechanical friction from tight clothing, physical activity, and body weight distribution in skinfold areas directly triggers HS flares. Shaving in affected areas can precipitate follicular disruption and new lesion formation.
Diet may also influence HS activity, with some patients reporting improvements after reducing dairy intake or following low-glycaemic diets. However, robust clinical evidence for specific dietary interventions remains limited, and dietary changes should complement rather than replace established medical treatments.
Recognising the Symptoms of Hidradenitis Suppurativa
HS symptoms range considerably in severity from mild and intermittent to severe, constant, and functionally disabling. The condition follows a relapsing and remitting course in most patients, with periods of relative calm interrupted by painful acute flares.
Pain is the most consistently reported and impactful symptom across all disease stages. HS pain is not merely superficial; it involves deep, throbbing, burning discomfort that significantly restricts movement and daily functioning.
Early-Stage Symptoms
Early HS typically presents as single, painful, deep nodules resembling boils in characteristic body areas. These nodules may resolve partially between episodes, leaving behind subtle thickening or discolouration of the overlying skin.
Many patients describe months or years of these single, intermittent lesions before multiple simultaneous lesions appear. The early stage represents the optimal time for intervention, as permanent structural skin damage has not yet occurred.
Progression to Abscesses and Discharge
As disease progresses, nodules evolve into fluctuant abscesses that may rupture and discharge a mixture of pus, blood, and malodorous fluid. This discharge causes significant distress, practical difficulties with clothing and hygiene, and profound social embarrassment for affected individuals.
The characteristic odour associated with HS discharge results from secondary bacterial colonisation rather than primary infection. Staphylococcus epidermidis, anaerobic bacteria, and other skin commensals colonise existing lesions and intensify the inflammatory response within them.
Sinus Tracts and Scarring
Advanced HS develops interconnected tunnels beneath the skin surface called sinus tracts or fistulae. These tunnels connect multiple lesion sites, discharge chronically, and cause progressive, irreversible scarring of the affected skin areas.
Rope-like, cordlike scars and distorted skin architecture in affected body regions represent the lasting structural consequences of inadequately treated disease. Once sinus tracts and significant scarring develop, surgical intervention rather than medical treatment alone becomes necessary for satisfactory management.
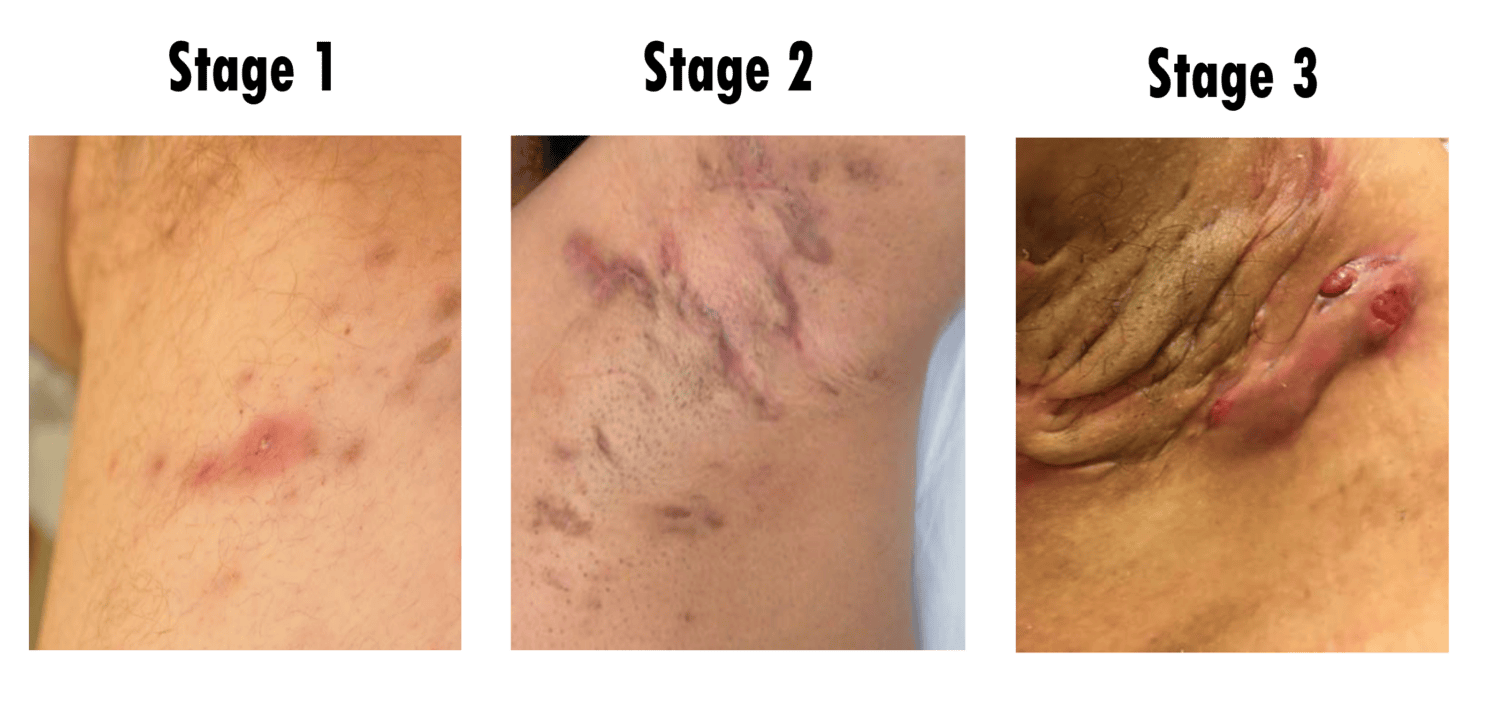
Staging Hidradenitis Suppurativa: The Hurley Classification
Dermatologists use the Hurley staging system to classify HS severity and guide treatment decisions. This three-stage classification system helps communicate disease extent and select the most appropriate treatment approach for each patient.
Hurley Stage I describes single or multiple isolated abscesses without sinus tract formation or significant scarring. Stage II involves recurrent abscesses with some sinus tract formation and scarring but with lesions remaining relatively separated.
Hurley Stage III and Beyond
Hurley Stage III represents the most severe form of HS, with multiple interconnected sinus tracts, abscesses, and extensive scarring affecting the entire anatomical region. This stage causes marked functional impairment, chronic pain, and profound negative impact on quality of life.
The International Hidradenitis Suppurativa Severity Score System (IHS4) provides a more nuanced assessment tool used increasingly in clinical practice and research settings. More detailed scoring allows better tracking of treatment response and disease progression over time.
Diagnosing Hidradenitis Suppurativa
HS diagnosis is entirely clinical, based on the characteristic history, lesion types, anatomical location, and disease course. No laboratory test or imaging study confirms or excludes the diagnosis independently.
The three diagnostic criteria are lesions in characteristic body areas, recurrence of lesions, and the presence of typical lesion types including nodules, abscesses, or sinus tracts. Meeting all three criteria confirms the diagnosis without the need for additional investigations.
Tests Used to Assess HS
Although no diagnostic test exists for HS itself, several investigations help assess disease severity, detect complications, and screen for associated conditions. Full blood count, inflammatory markers such as CRP and ESR, and metabolic screening are routinely performed.
Microbiological swabs of discharging lesions identify secondary bacterial colonisers and guide antibiotic selection when these contribute to disease activity. Imaging studies, including ultrasound of affected areas, help visualise deep sinus tract extension not apparent on surface examination.
Associated Conditions Requiring Assessment
HS is associated with several systemic conditions that require proactive screening and management. These include metabolic syndrome, type 2 diabetes, inflammatory bowel disease, and spondyloarthropathy.
Squamous cell carcinoma arising within long-standing sinus tracts represents a rare but serious complication of severe, chronic HS. Any rapidly growing, non-healing lesion within established HS disease warrants urgent biopsy to exclude this malignant transformation.
Medical Treatment of Hidradenitis Suppurativa
HS treatment follows a stepwise approach based on disease severity. Mild disease responds to topical treatments and lifestyle modifications, while moderate and severe disease requires systemic medications and often biological therapies.
No current treatment cures HS, and realistic treatment goals centre on reducing flare frequency and severity, managing pain, preventing progression, and preserving quality of life. Long-term specialist dermatology care underpins successful disease management across all severity levels.
Topical and Local Treatments
Topical clindamycin 1% lotion applied to affected areas twice daily reduces surface bacterial colonisation and mild inflammation. Clinical evidence supports its use as monotherapy for Hurley Stage I disease.
Intralesional triamcinolone injections directly into individual nodules provide rapid anti-inflammatory effects and help abort early lesion development. These injections work best when given early in a flare before full abscess formation occurs.
Systemic Antibiotic Therapy
Oral antibiotic combinations, most commonly tetracycline antibiotics or rifampicin combined with clindamycin, target both bacterial colonisation and the anti-inflammatory properties of these drug classes. Extended courses of three to six months provide disease control in moderate HS.
Antibiotic therapy does not cure HS and typically produces improvement rather than complete remission. Disease activity frequently returns after antibiotic discontinuation, necessitating alternative maintenance strategies for long-term disease control.
Hormonal Therapies
Anti-androgenic treatments including combined oral contraceptives, spironolactone, and finasteride reduce HS activity in some patients by modulating the hormonal drive to follicular occlusion. These options are particularly relevant for people whose disease clearly worsens with hormonal fluctuations.
Hormonal therapy works best as part of a combined treatment strategy rather than as sole management. Specialist guidance ensures appropriate patient selection and monitoring for side effects during hormonal treatment courses.
Biological and Advanced Systemic Treatments for HS
Moderate to severe HS that does not respond to conventional treatments requires biological therapy. These targeted medications have transformed outcomes for patients with advanced disease who previously had very limited effective options.
Specialist dermatology assessment, thorough disease documentation, and appropriate safety screening precede biological therapy initiation. Regular monitoring for treatment response and adverse effects continues throughout the treatment course.
Adalimumab: The First Approved Biological for HS
Adalimumab, a TNF-α inhibitor, is the first and currently most widely approved biological therapy for moderate to severe hidradenitis suppurativa. It reduces inflammatory signalling that drives painful lesion formation and disease progression.
The pivotal PIONEER I and II clinical trials demonstrated that adalimumab significantly reduced active lesion counts and pain scores compared to placebo. Adalimumab is given by subcutaneous injection weekly and achieves clinical response in approximately 50% of treated patients.
Secukinumab and IL-17 Inhibition
Secukinumab, which targets the IL-17A inflammatory pathway, received regulatory approval for moderate to severe HS based on positive phase III clinical trial results. IL-17 inhibition addresses a different but equally important inflammatory pathway from TNF-α blockade.
Secukinumab provides an effective alternative for patients who do not respond adequately to adalimumab or who experience loss of response over time. Combining different biological mechanisms in sequence or considering combination approaches forms an active area of ongoing clinical research.
Emerging Treatments and Future Directions
Several new biological and small molecule therapies are progressing through clinical trials for HS. Bimekizumab, which targets both IL-17A and IL-17F simultaneously, has demonstrated particularly strong efficacy signals in early trial data.
JAK inhibitors, which block multiple inflammatory pathways simultaneously, also show promise for HS treatment. The expanding treatment pipeline offers genuine hope for patients who currently achieve only partial responses with available therapies.
Surgical Management of Hidradenitis Suppurativa
Surgery plays an essential role in HS management, particularly for advanced disease with established sinus tracts and scarring that medications alone cannot adequately address. The surgical approach must match the extent and stage of disease to achieve meaningful results.
Deroofing, which involves surgically unroofing individual sinus tracts and allowing them to heal by secondary intention, effectively treats localised tunnel disease. Local anaesthetic deroofing produces durable results with low recurrence rates in appropriately selected lesions.
Wide Local Excision
Wide local excision removes all affected skin and subcutaneous tissue from an entire anatomical region. This aggressive approach achieves the lowest recurrence rates of any surgical technique but creates significant wounds requiring complex reconstruction.
Healing after wide excision may occur by secondary intention, skin grafting, or flap reconstruction depending on wound size and location. Plastic surgery involvement ensures the best functional and cosmetic outcomes after major HS excision procedures.
Laser and Minimally Invasive Procedures
Laser hair removal in HS-affected areas reduces hair follicle density and thereby decreases the substrate for follicular occlusion. Nd:YAG laser treatment shows the strongest evidence base among laser modalities for HS and reduces lesion counts meaningfully.
Carbon dioxide laser ablation of sinus tracts offers a minimally invasive surgical option with good efficacy for localised disease. These procedures are increasingly available in specialist HS centres and provide valuable treatment options for patients unsuitable for major surgery.
The Psychological Burden of Hidradenitis Suppurativa
The impact of hidradenitis suppurativa extends profoundly beyond the physical symptoms of pain and discharge. HS consistently ranks among the skin conditions with the most severely impaired quality of life in comparative dermatological studies.
Depression and anxiety affect the majority of people with moderate to severe HS. Chronic pain, social isolation, body image disturbance, and the unpredictability of flares all contribute to significant psychological burden throughout the disease course.
Social and Occupational Consequences
Many people with HS avoid social situations, intimate relationships, exercise, and certain occupational activities due to pain, discharge, and odour associated with their condition. This withdrawal further compounds depression and reduces quality of life beyond the direct disease effects.
The diagnostic delay of seven to ten years means many patients spend formative years of their lives suffering without explanation, validation, or effective treatment. Receiving a correct diagnosis itself often brings significant psychological relief by providing a framework for understanding their experience.
Accessing Psychological Support
Psychological support should form an integral part of comprehensive HS care rather than an optional add-on. Cognitive behavioural therapy, peer support groups, and specialist nurses skilled in chronic skin disease management all contribute meaningfully to psychological wellbeing.
Patient advocacy organisations such as the HS Foundation provide community connection, educational resources, and advocacy for improved healthcare access. These peer networks provide a form of understanding and validation that clinical consultations alone cannot always supply.
Frequently Asked Questions About Hidradenitis Suppurativa
What causes hidradenitis suppurativa to develop?
Hidradenitis suppurativa develops through a combination of follicular occlusion, immune system dysregulation, genetic predisposition, and hormonal influences. Hair follicles in affected areas become blocked and rupture, triggering intense inflammatory responses that cause painful nodules, abscesses, and sinus tracts. Factors such as obesity, smoking, and friction in skin fold areas worsen disease severity but do not independently cause HS in the absence of underlying susceptibility.
Why does hidradenitis suppurativa take so long to diagnose?
The long diagnostic delay occurs because HS lesions closely resemble ordinary boils, recurrent skin infections, and folliculitis, which clinicians without specialist dermatology training frequently misidentify. Patients often consult multiple healthcare providers over many years before receiving a correct diagnosis. Raising awareness of the characteristic pattern of recurrent lesions in specific body locations is essential for reducing this diagnostic delay significantly.
Is hidradenitis suppurativa contagious or caused by poor hygiene?
Hidradenitis suppurativa is neither contagious nor caused by poor hygiene. It results from genetic, immunological, and hormonal factors entirely beyond an individual’s control. This misconception causes considerable shame and delays help-seeking in many affected people. Vigorous scrubbing or antiseptic washing of affected areas can actually worsen HS by causing additional skin trauma and irritation.
Can hidradenitis suppurativa be cured with surgery?
Wide surgical excision of affected regions achieves the lowest recurrence rates of any current treatment and provides durable relief for many patients with advanced disease. However, HS is a systemic inflammatory condition, meaning new lesions can develop outside surgically treated areas over time. Surgery represents an important component of comprehensive HS management rather than a standalone cure, and most patients benefit from combining surgical and medical treatment approaches.
What lifestyle changes help manage hidradenitis suppurativa?
Smoking cessation, achieving and maintaining a healthy body weight, wearing loose-fitting clothing, avoiding shaving in affected areas, and reducing friction in skinfold regions all reduce HS flare frequency and severity. Some patients experience improvement with dietary modifications including low-dairy or low-glycaemic diets, though evidence remains limited. These lifestyle measures work most effectively as adjuncts to appropriate medical and surgical treatment rather than replacements for specialist dermatological care.
Ending the Years of Misdiagnosis and Suffering From HS
Hidradenitis suppurativa remains one of dermatology’s most underdiagnosed, undertreated, and misunderstood conditions. Yet it causes suffering comparable to the most severe chronic diseases across any medical specialty.
The expanding landscape of biological therapies, improved surgical techniques, and growing specialist awareness is transforming what is achievable for people living with HS. Patients who once had few effective options now have access to treatments that can dramatically reduce their lesion burden, pain, and impact on daily life.
Most urgently, reducing the seven-to-ten-year diagnostic delay requires broader education among healthcare professionals and greater public awareness of HS as a distinct, serious, and highly treatable inflammatory disease. Every year that passes without a correct diagnosis is a year of avoidable pain, progressive skin damage, and unnecessary psychological suffering that no patient should have to endure.
Disclaimer:
This article is intended for general informational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for any medical concerns.
References:
- In December 2000, the United Nations General Assembly established the day to raise awareness about the importance of biodiversity.
- Biological therapeutics, known as biologicals, represent a revolutionary class of medicines fundamentally different from traditional pharmaceuticals.
- Inflammatory bowel disease is a group of chronic autoimmune inflammatory conditions affecting the digestive tract. The two main forms are Crohn’s disease
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.