
Rotator Cuff Tear: Symptoms, Diagnosis, and When to Have Surgery
he shoulder is the most mobile joint in the human body. It can swing forward, reach overhead, rotate inward and outward, and extend backward — all with remarkable speed and power. This extraordinary range of movement depends on a group of four muscles and their tendons working together in perfect coordination. When any part of this group tears, the consequences can be painful, disabling, and surprisingly difficult to resolve without the right treatment.
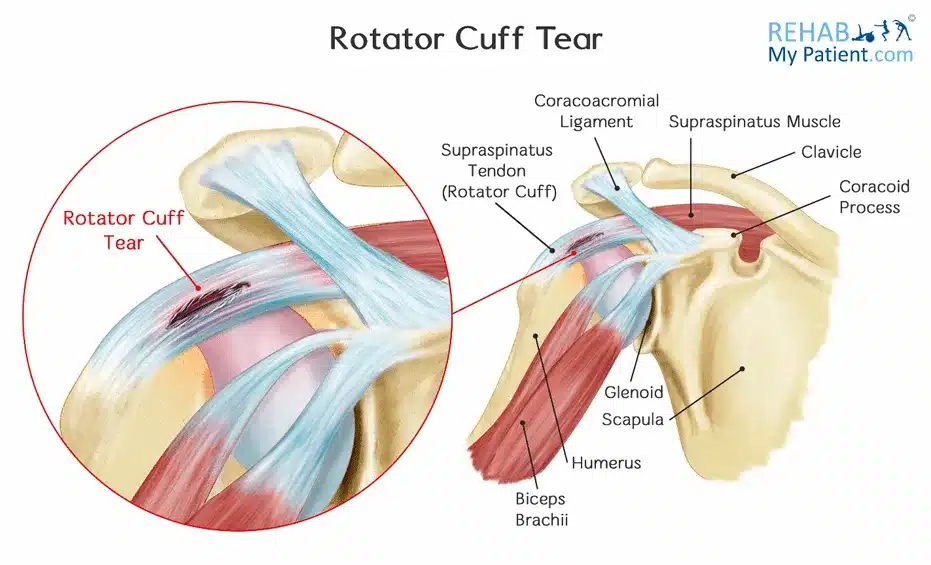
The rotator cuff is the collective name for the four muscles — and their tendons — that surround and stabilise the shoulder joint. These tendons attach the muscles to the head of the humerus — the upper arm bone — and hold it firmly in the shoulder socket while allowing all that extraordinary movement. When one or more of these tendons tears — either partially or completely — the result is weakness, pain, and restricted function that can range from a minor nuisance to a completely disabling injury.
Rotator cuff tear symptoms diagnosis surgery is the central focus of this article. Furthermore, many people who discover they have a rotator cuff tear immediately assume they need an operation. However, the evidence shows that surgery is not always the best or first option — and that the right decision depends on multiple factors that deserve careful evaluation. Consequently, understanding the full picture of rotator cuff tears — what they are, how they feel, and when surgery genuinely adds value — gives patients the confidence to make informed choices about their shoulder care.
Quick Answer
A rotator cuff tear is a partial or complete tear of one or more tendons surrounding the shoulder joint. It causes shoulder pain, weakness, and restricted movement. Diagnosis uses clinical examination and MRI. Many tears respond well to physiotherapy and injections without surgery. Surgery works best for complete tears in active younger patients or those who fail conservative care.
What Is the Rotator Cuff?
The Four Muscles and Their Roles
The rotator cuff consists of four muscles — supraspinatus, infraspinatus, teres minor, and subscapularis. Each muscle originates from the shoulder blade and attaches to the head of the humerus through its own tendon. Together, they compress the humeral head into the shallow shoulder socket — called the glenoid — providing dynamic stability during every arm movement.
The supraspinatus is the most commonly injured tendon. It runs across the top of the shoulder and initiates the first 30 degrees of arm elevation away from the body. The infraspinatus and teres minor sit at the back of the shoulder and rotate the arm outward. The subscapularis covers the front of the shoulder blade and rotates the arm inward. Furthermore, all four tendons converge into a single broad sheet of tissue — the rotator cuff — that blends with the joint capsule and covers the humeral head like a cuff around a sleeve. Consequently, a tear in any tendon disrupts the entire coordinated system.
Why Rotator Cuff Tendons Tear
Rotator cuff tendons tear through two main mechanisms. Acute tears result from a sudden forceful injury — such as a fall onto an outstretched hand, a sudden heavy pull, or a shoulder dislocation. Degenerative tears — by far the more common type — develop gradually over years as the tendons weaken, fray, and eventually rupture from the cumulative effects of ageing, reduced blood supply, and repetitive microtrauma.
The critical zone of the supraspinatus tendon — approximately one centimetre from its attachment to the humerus — is particularly vulnerable because it receives relatively poor blood supply. Consequently, this area heals poorly when damaged and is the site where the majority of rotator cuff tears begin and progress. For context on how blood supply affects musculoskeletal tissue survival, see our article on avascular necrosis — when bone tissue dies from lack of blood supply.
Types of Rotator Cuff Tears
Partial Thickness Tears
Partial thickness tears involve damage to part of the tendon without complete disruption of the entire thickness from top to bottom. They are further classified by location — bursal-side tears affect the upper surface of the tendon adjacent to the bursa — a fluid-filled sac overlying the tendon — while articular-side tears affect the lower surface adjacent to the joint. Furthermore, intrasubstance tears occur within the body of the tendon without breaking either surface.
Partial tears vary considerably in their depth — from minor fraying involving less than 25% of tendon thickness to high-grade partial tears involving more than 50% of tendon thickness. Moreover, high-grade partial tears behave clinically more like complete tears — causing significant weakness and pain — and carry a higher risk of progressing to complete rupture without treatment. Consequently, the grade of a partial tear directly influences whether conservative management or surgical repair is more appropriate.
Full Thickness Tears
Full thickness tears extend completely through the tendon from the articular surface to the bursal surface — creating a hole through which fluid and tissue can communicate between the joint and the bursa. Small full thickness tears measure less than one centimetre. Medium tears measure one to three centimetres. Large tears measure three to five centimetres. Massive tears involve more than five centimetres or affect two or more tendons simultaneously.
Massive tears frequently involve retraction — the torn tendon recoils away from its attachment, pulled by the contracting muscle. Furthermore, fatty infiltration — replacement of muscle fibres with fat — develops in the muscle belly when the tendon has been torn for a prolonged period. Consequently, massive tears with significant retraction and fatty infiltration present the most challenging surgical scenarios and the most uncertain outcomes after repair.
Symptoms of Rotator Cuff Tears
Pain Patterns
Rotator cuff tear symptoms diagnosis surgery begins with recognising the characteristic pain pattern. Shoulder pain is the defining symptom and typically has several distinctive features that help distinguish rotator cuff pathology from other causes of shoulder discomfort. The pain most commonly affects the outer aspect of the shoulder — over the deltoid muscle — and often radiates down the outside of the upper arm toward the elbow. However, it rarely extends below the elbow, which helps distinguish it from cervical spine nerve root compression.
Night pain is a particularly characteristic feature of rotator cuff tears. Many patients describe being woken by shoulder pain when lying on the affected side, or experiencing a deep aching pain in the shoulder during the night even when lying on the unaffected side. Furthermore, the pain worsens with reaching overhead, reaching behind the back, lifting objects away from the body, and any activity that requires sustained shoulder elevation. Consequently, activities such as dressing, reaching into high cupboards, and throwing become painful and restricted.
A painful arc — pain occurring between 60 and 120 degrees of arm elevation — is a clinical hallmark of supraspinatus pathology. As the arm reaches this range, the supraspinatus tendon passes under the acromion — the bony roof of the shoulder — and an injured or torn tendon causes pain during this passage. Furthermore, pain often reduces above 120 degrees as the tendon clears the acromion — a pattern that helps clinicians distinguish rotator cuff pain from other causes of shoulder dysfunction.
Weakness and Functional Limitation
Weakness is the second defining symptom of rotator cuff tears. It reflects both the mechanical deficit caused by tendon discontinuity and the pain inhibition that prevents full muscle activation. Supraspinatus tears cause weakness in shoulder abduction — raising the arm to the side. Infraspinatus and teres minor tears cause weakness in external rotation — rotating the arm outward. Subscapularis tears cause weakness in internal rotation and the ability to press the hand against the abdomen.
In massive tears, the arm may fall limply to the side despite the patient’s best efforts to maintain elevation — a finding called a positive drop arm test. Moreover, complete subscapularis tears can produce anterior shoulder instability — the humeral head slips forward within the socket because the subscapularis tendon normally prevents this movement. Consequently, assessing specific rotator cuff muscle strength — not just overall shoulder movement — is essential for localising the tear and planning treatment.
How Doctors Diagnose Rotator Cuff Tears
Clinical Examination
Diagnosing rotator cuff tear symptoms diagnosis surgery begins with a structured clinical examination. Several specific tests — each targeting a different rotator cuff muscle — help clinicians localise the tear with reasonable accuracy before imaging.
The empty can test — or Jobe’s test — assesses supraspinatus integrity. The examiner elevates the patient’s arm to 90 degrees in the scapular plane with the thumb pointing downward and applies downward resistance. Weakness or pain indicates supraspinatus pathology. The external rotation lag sign detects large infraspinatus tears — a positive test shows the patient cannot maintain passive external rotation once the examiner releases the wrist. The lift-off test and belly-press test assess subscapularis integrity — a positive test shows inability to maintain the hand pressed against the abdomen against resistance.
Furthermore, impingement tests — including Neer’s sign and Hawkins-Kennedy test — identify subacromial impingement that commonly coexists with rotator cuff pathology. Consequently, combining multiple specific tests produces better diagnostic accuracy than any single test in isolation.
Imaging Studies
Plain X-ray of the shoulder provides important baseline information but cannot directly visualise soft tissue structures including tendons. However, X-ray reveals secondary signs of chronic rotator cuff disease — including superior migration of the humeral head toward the acromion when large cuff tears allow the deltoid to pull the humerus upward unopposed, acromial spurs that impinge on the supraspinatus tendon, and glenohumeral arthritis that may influence treatment decisions.
MRI is the gold standard imaging investigation for rotator cuff tears. It directly visualises all four rotator cuff tendons, quantifies tear size and retraction, assesses muscle quality — identifying fatty infiltration — and evaluates the biceps tendon and labrum simultaneously. Furthermore, MRI helps distinguish partial from full thickness tears and localises tears precisely within the tendon footprint. Consequently, MRI findings directly guide both the decision about whether to operate and the specific surgical technique required.
Ultrasound is an accessible, real-time, and cost-effective alternative to MRI for experienced musculoskeletal sonographers. In skilled hands, dynamic ultrasound examination achieves diagnostic accuracy comparable to MRI for full thickness supraspinatus tears. Moreover, ultrasound allows guided injection into the subacromial space in the same session as the diagnostic evaluation. However, it is more operator-dependent than MRI and less reliable for detecting partial tears and evaluating muscle quality.
Treatment of Rotator Cuff Tears
Physiotherapy — The Essential First Step
Physiotherapy is the cornerstone of initial management for the majority of rotator cuff tears — including many complete tears. The evidence consistently shows that outcomes from physiotherapy are equivalent to surgical repair for a significant proportion of patients — particularly those with degenerative tears, older age, lower activity demands, and tears without significant weakness.
A structured physiotherapy programme for rotator cuff tears focuses on several key goals. Restoring full passive shoulder range of movement prevents the secondary stiffness — called adhesive capsulitis — that frequently develops when a painful shoulder is protected and immobilised. Strengthening the intact rotator cuff muscles compensates for the torn tendon by improving dynamic shoulder stability. Furthermore, strengthening the periscapular muscles — the muscles controlling shoulder blade position — optimises the mechanical environment of the shoulder joint and reduces impingement stress on the remaining tendon tissue.
Pain management supports engagement with physiotherapy. Subacromial corticosteroid injection — delivering anti-inflammatory medication directly into the subacromial space — significantly reduces pain and allows patients to participate fully in rehabilitation. However, repeated injections should be limited — most guidelines recommend no more than three injections per shoulder per year — because high cumulative steroid doses impair tendon healing and increase the risk of tendon rupture. For context on how chronic pain conditions interact with shoulder rehabilitation, see our article on fibromyalgia — the pain condition that is real, widely misunderstood, and treatable.
When Surgery Is Actually Needed
The decision to recommend surgery for a rotator cuff tear requires careful individualised assessment. Surgery is not automatically the right choice for every tear — and the evidence supports conservative management as a genuinely effective alternative for many patients. However, surgery is clearly indicated in specific circumstances.
Acute complete tears in younger, active patients — particularly those who tore their tendon during a single traumatic event rather than through degeneration — benefit most from early surgical repair. In young active people, the torn tendon ends retract quickly and the muscle begins to undergo fatty infiltration within weeks to months. Consequently, delay in repair significantly worsens the biological quality of the tissue available for reconstruction and reduces the probability of a successful outcome.
Persistent symptoms despite three to six months of structured physiotherapy represent the most common indication for surgery in patients with degenerative tears. If pain, weakness, and functional limitation remain significant after a genuinely committed physiotherapy programme, surgical repair becomes a reasonable next step. Furthermore, patients with high functional demands — athletes, manual labourers, and overhead workers — may tolerate residual weakness and pain less well than sedentary individuals. Consequently, their threshold for surgical intervention may reasonably be lower.
Surgical Techniques
Arthroscopic rotator cuff repair has largely replaced open surgery over the past two decades. Small cameras and instruments are inserted through keyhole incisions — typically two to four portals of five to ten millimetres each — to visualise the tear, prepare the tendon footprint on the humerus, and secure the torn tendon back to the bone using metal or bioabsorbable anchors with attached sutures.
Furthermore, arthroscopic surgery allows simultaneous treatment of associated pathology — including biceps tendon disease, labral tears, and acromioplasty — in the same session. Recovery after arthroscopic repair involves six weeks in a sling, followed by progressive physiotherapy over four to six months. Return to full overhead activity and sport typically takes six to twelve months after repair of large tears. Consequently, patients must understand and commit to this extended recovery period before deciding to proceed with surgery.
For context on how bone quality affects anchor fixation strength and surgical outcomes in rotator cuff repair, see our article on osteoporosis — how bones lose density and what reverses it.
Recovery and Long-Term Outcomes
Post-Operative Rehabilitation
Successful rotator cuff repair depends as much on rehabilitation as on surgical technique. The initial six weeks after surgery focus on protecting the repair while it heals — wearing a sling, performing pendulum exercises, and allowing only passive movement within limits set by the surgeon. Furthermore, the tendon-to-bone healing process takes approximately twelve weeks to complete structural maturation — making premature loading the most common cause of re-tear.
Active-assisted and then active range of movement exercises begin after six weeks. Strengthening exercises start progressively from twelve weeks onward as healing matures. Furthermore, sport-specific or work-specific rehabilitation begins from four to six months depending on the size of the repair and the demands of the activity. Consequently, full return to demanding overhead activities takes most patients nine to twelve months after large tear repairs.
Managing Non-Operative Tears Long Term
People who manage rotator cuff tears non-operatively require ongoing attention to shoulder strength and function throughout their lives. Regular physiotherapy review ensures exercise programmes remain appropriate as shoulder demands and tear characteristics evolve. Moreover, avoiding sustained overhead loading and heavy repetitive lifting reduces the risk of tear progression.
Annual or biennial reassessment — with repeat imaging if symptoms change significantly — monitors for tear enlargement that might shift the treatment balance toward surgery. For context on managing degenerative musculoskeletal conditions that frequently coexist with rotator cuff disease in older adults, see our article on osteoarthritis — inflammation, causes, and what actually helps — and spondylolisthesis — slipped vertebra, back pain, and treatment.
When to Seek Medical Help
See a doctor promptly if you develop acute severe shoulder pain after a fall or sudden injury — particularly if the pain is accompanied by immediate weakness in raising the arm. Furthermore, seek medical attention if shoulder pain persists for more than four to six weeks, significantly restricts daily activities, disrupts sleep on multiple nights each week, or fails to improve with simple analgesics and rest.
Consequently, early clinical assessment and appropriate imaging allow an accurate diagnosis and a treatment plan tailored to the specific tear characteristics — giving the shoulder the best possible chance of recovery whether surgery is ultimately needed or not.
Frequently Asked Questions
1. Can a rotator cuff tear heal without surgery?
Partial tears and small full thickness tears can achieve clinical healing — reduction in pain and recovery of function — without surgery in many patients through physiotherapy and time. However, the structural tear itself rarely closes completely without surgical repair. Furthermore, large complete tears can worsen over time without repair. Consequently, the relevant question for most patients is not whether the tendon heals but whether function and pain improve sufficiently to meet their daily needs without an operation.
2. How long does recovery take after rotator cuff surgery?
Recovery after arthroscopic rotator cuff repair typically spans six to twelve months for large tears. The first six weeks involve sling immobilisation. Physiotherapy then progressively restores movement, strength, and function over the following months. Furthermore, the re-tear rate is higher in the first twelve months when tissue healing is still maturing. Consequently, returning to full overhead sport or heavy manual work before twelve months significantly increases the risk of repair failure.
3. What happens if a rotator cuff tear goes untreated?
Small and partial tears often remain stable for years without treatment. However, untreated complete tears — particularly in younger, active people — tend to enlarge progressively. As the tear grows, the tendon retracts and the muscle undergoes fatty infiltration — permanently replacing functional muscle with fat that cannot contract. Moreover, massive irreparable tears eventually cause rotator cuff arthropathy — a severe form of shoulder arthritis with humeral head collapse. Consequently, monitoring and appropriate timely treatment prevent the worst long-term outcomes.
4. Is physiotherapy enough for a complete rotator cuff tear?
For many patients — particularly older adults with degenerative complete tears and lower physical demands — physiotherapy produces outcomes equivalent to surgical repair in clinical trials. However, younger patients, those with acute traumatic tears, and those with significant ongoing weakness despite physiotherapy achieve better long-term results with surgery. Furthermore, physiotherapy requires genuine commitment — typically three to six months of regular sessions and home exercises. Consequently, the success of conservative management depends heavily on patient compliance and the quality of the rehabilitation programme.
5. Can a rotator cuff tear come back after surgery?
Yes. Re-tear after surgical repair occurs in a significant proportion of patients — ranging from roughly 15% for small tears to more than 50% for massive tears in some series. However, many patients who experience a structural re-tear still report satisfactory pain relief and functional improvement compared with their pre-operative state. Furthermore, factors including tear size, tissue quality, patient age, and rehabilitation compliance all influence re-tear risk. Consequently, a re-tear on imaging does not automatically mean the surgery has failed or that further surgery is required.
References
- Psoriatic Arthritis has multiple patterns of joint involvement. Understanding the different patterns helps with diagnosis and guides treatment.
- IndiGo, which holds more than 60% of the domestic aviation market share, is currently facing one of its most severe operational crises.
- This amendment not only aims to ease the financial burden on expressway users but also focuses on environmental benefits.
Disclaimer
This article adapts publicly available information from WHO’s Musculoskeletal Conditions page. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform and not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.