
Osteoporosis: How Bones Lose Density and What Can Actually Reverse It
Bones look solid and unchanging from the outside. However, inside every bone in the body, a constant process of breaking down and rebuilding is happening around the clock. This process keeps bones strong, repairs tiny damage, and adjusts bone structure in response to the forces placed on it. When this balance tips in the wrong direction — when bones break down faster than they rebuild — density falls and bones become dangerously fragile.
Osteoporosis is a condition in which bones lose so much density that they become weak enough to fracture from minor falls, bumps, or even everyday movements like bending or coughing. It is often called a silent disease because it causes no pain and no obvious symptoms until a bone actually breaks. By that point, significant and permanent bone loss has already occurred.
Osteoporosis bones lose density reverse is the central question this article addresses — how bones weaken, who is most at risk, and critically, what modern medicine and lifestyle science can actually do to rebuild bone strength and reduce fracture risk. Furthermore, understanding osteoporosis clearly gives people the power to act before a fracture happens rather than after. Consequently, early awareness and proactive management can be genuinely life-changing for millions of people worldwide.
Quick Answer
Osteoporosis is a condition in which bones gradually lose density and become fragile enough to fracture easily. It results from an imbalance between the cells that build new bone and those that break it down. Treatment combining medications, calcium, vitamin D, and weight-bearing exercise can slow bone loss and in some cases meaningfully increase bone density.
How Bones Normally Stay Strong
The Bone Remodelling Cycle
Bone is living tissue. It constantly renews itself through a process called bone remodelling. Two types of cells carry out this process. Osteoclasts — cells that break down old or damaged bone — remove small sections of bone tissue continuously. Osteoblasts — cells that build new bone — then fill the spaces left behind with fresh, mineralised tissue.
In a healthy young adult, these two cell types stay in balance. Osteoblasts produce bone at roughly the same rate as osteoclasts remove it. As a result, bone density remains stable and the skeleton maintains its strength and structure. Peak bone mass — the maximum density bones can achieve — develops by the late twenties in most people. Consequently, the higher the peak bone mass a person builds during youth, the more bone loss they can afford later in life before the fragility threshold is reached.
When the Balance Tips
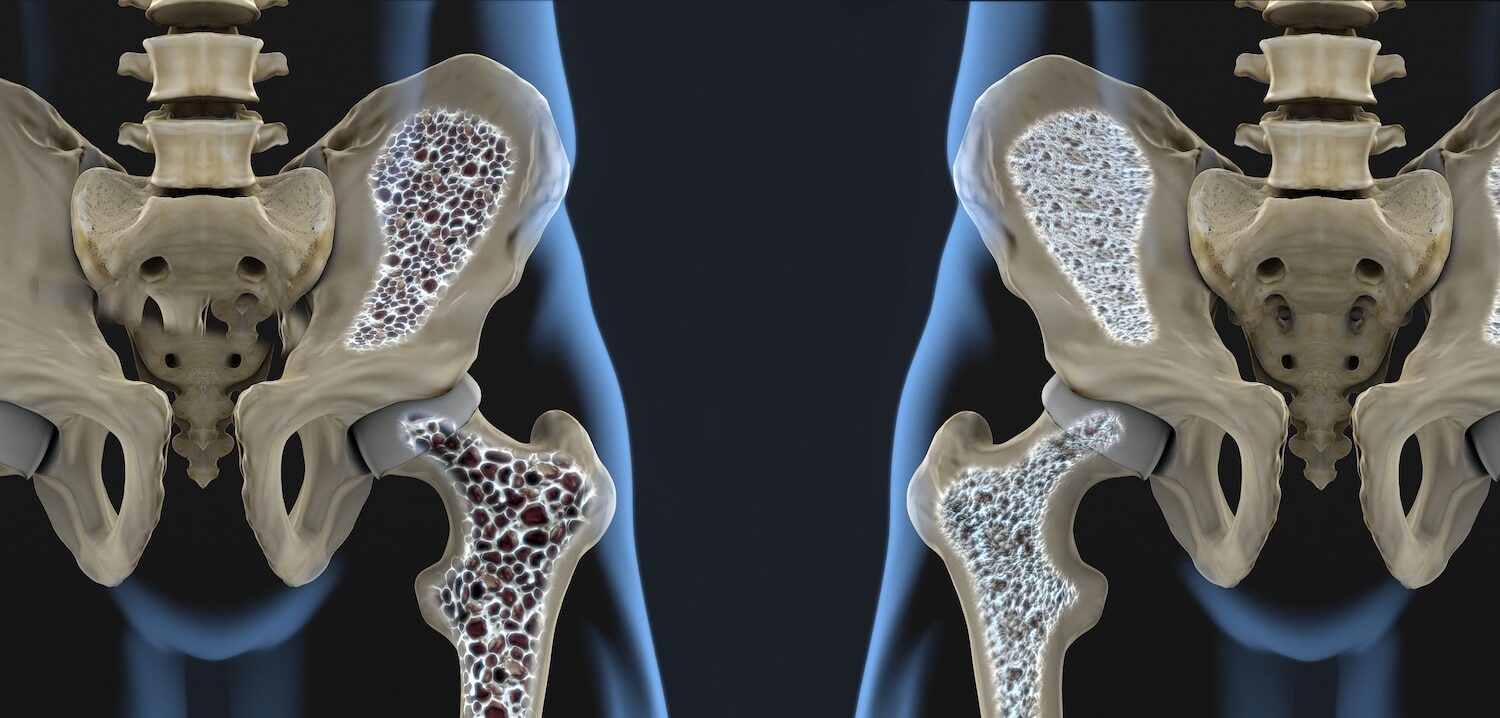
After the age of 30, bone remodelling naturally shifts slightly in favour of breakdown over rebuilding. This gradual net loss of bone is a normal part of ageing. However, in some people, this shift becomes dramatic. Osteoclast activity significantly outpaces osteoblast activity — stripping away bone tissue faster than it can be replaced.
Over years and decades, this imbalance hollows out the internal structure of bones, replacing the dense, interconnected scaffolding of healthy bone with a porous, fragile structure resembling a sponge with large holes. Consequently, bones that once withstood significant force can fracture from minimal trauma — a condition doctors call fragility fracture. For context on how hormonal and metabolic conditions affect bone health alongside kidney function, see our article on chronic kidney disease — stages, symptoms, and how to slow the decline.
What Causes Osteoporosis?
Hormonal Changes
Osteoporosis bones lose density reverse begins with understanding its causes. Hormonal changes are the most powerful driver of bone loss in most people. Oestrogen — a hormone produced primarily in the ovaries — plays a critical protective role in bone by restraining osteoclast activity. When oestrogen levels fall sharply after menopause, this restraint is removed. As a result, osteoclasts become significantly more active and bone loss accelerates dramatically.
In the first five to ten years after menopause, some women lose up to 20% of their bone density. This rapid loss explains why osteoporosis is far more common in postmenopausal women than in any other group. Furthermore, it explains why early menopause — whether natural or surgical — significantly increases lifetime osteoporosis risk.
In men, testosterone plays a similar protective role. Testosterone levels fall gradually with age rather than sharply, which is why men develop osteoporosis later than women and at lower rates. However, men with significantly low testosterone — called hypogonadism — face a substantially elevated osteoporosis risk. Moreover, men are often underdiagnosed because osteoporosis is incorrectly perceived as a women’s disease.
Medical Conditions and Medications
Several medical conditions accelerate bone loss beyond the normal rate of ageing. Autoimmune conditions — including rheumatoid arthritis and lupus — cause chronic inflammation that directly stimulates osteoclast activity. For context on how autoimmune conditions affect multiple body systems simultaneously, see our articles on lupus nephritis — when lupus attacks the kidneys — and membranous nephropathy — autoimmune kidney disease and its proteinuria.
Chronic kidney disease reduces the kidneys’ ability to activate vitamin D, impairs calcium absorption, and drives a hormonal cascade — called secondary hyperparathyroidism — that strips calcium from bones to maintain blood levels. Consequently, bone disease is a recognised and serious complication of advanced kidney disease. Coeliac disease, inflammatory bowel disease, and conditions causing malabsorption reduce calcium and vitamin D absorption from food. Hyperthyroidism and hyperparathyroidism — overactivity of the thyroid and parathyroid glands — accelerate bone breakdown directly.
Medications represent another critical risk category. Long-term corticosteroid use — such as prednisolone for asthma, rheumatoid arthritis, or inflammatory bowel disease — is the most common drug cause of osteoporosis. Corticosteroids suppress osteoblast activity and increase osteoclast activity simultaneously. Furthermore, anticonvulsants, proton pump inhibitors, and certain cancer hormone therapies all contribute to bone density loss with prolonged use.
Lifestyle Risk Factors
Several modifiable lifestyle factors significantly influence bone density. Low calcium and vitamin D intake during childhood and young adulthood reduces peak bone mass — the foundation upon which later bone health depends. Physical inactivity removes the mechanical stimulation that bones need to maintain density. Smoking reduces oestrogen levels and impairs blood supply to bone tissue. Moreover, excessive alcohol intake directly suppresses osteoblast activity and increases fall risk.
Low body weight — particularly a body mass index below 19 — is an independent risk factor because less mechanical loading reduces the stimulus for bone formation. In addition, a history of eating disorders — which frequently involve severe nutritional deficiency over extended periods — significantly compromises lifetime bone density.
Symptoms and Diagnosis of Osteoporosis
The Silent Nature of Bone Loss
Osteoporosis earns its description as a silent disease because it causes absolutely no symptoms during the years of progressive bone density loss. Pain, stiffness, and visible deformity do not appear until a fracture occurs. Furthermore, even some fractures — particularly vertebral fractures in the spine — can happen without any dramatic event, causing only mild back pain that is easily attributed to muscle strain.
The classic fracture sites for osteoporosis are the hip, spine, and wrist — though any bone can fracture. Hip fractures are the most serious consequence of osteoporosis. They require surgery, cause prolonged disability, and carry a 20 to 30% risk of death within one year in older adults. Spinal fractures — called vertebral compression fractures — cause loss of height and the characteristic forward-bending posture sometimes called a dowager’s hump. Consequently, any person who has lost more than two centimetres in height deserves a spine assessment.
DEXA Scan and Fracture Risk Assessment
The DEXA scan — dual-energy X-ray absorptiometry — is the standard diagnostic test for osteoporosis. It measures bone mineral density at the hip and spine and produces a T-score — a number comparing the person’s bone density to that of a healthy young adult at peak bone mass. A T-score of minus 1.0 or above is normal. A score between minus 1.0 and minus 2.5 indicates osteopenia — reduced bone density that has not yet reached the osteoporosis threshold. A score of minus 2.5 or below confirms osteoporosis.
FRAX — the Fracture Risk Assessment Tool — combines DEXA results with clinical risk factors to calculate a person’s ten-year probability of a major fracture. Furthermore, FRAX helps doctors decide who needs treatment even when DEXA scores fall in the borderline range. Consequently, the combination of DEXA and FRAX provides a more complete picture of fracture risk than bone density measurement alone.
Treatment: What Can Actually Reverse Bone Loss
Calcium and Vitamin D — The Foundation
Treating osteoporosis bones lose density reverse begins with ensuring adequate calcium and vitamin D. These two nutrients are the raw materials of bone mineralisation. Adults over 50 need roughly 1,200 milligrams of calcium per day — ideally from dietary sources including dairy products, fortified plant milks, leafy green vegetables, tofu, and almonds. Supplements fill the gap when diet alone falls short. However, calcium supplements should be taken with food and limited to 500 milligrams per dose to maximise absorption and minimise cardiovascular risk.
Vitamin D enables the gut to absorb calcium efficiently. Without adequate vitamin D, even a calcium-rich diet fails to mineralise bone effectively. Adults at risk of osteoporosis typically need 800 to 1,000 international units of vitamin D daily. Moreover, sunlight exposure — 15 to 30 minutes on the forearms and face on most days — supports vitamin D production in the skin. Consequently, people with limited sun exposure, dark skin, or chronic illness often need supplements to maintain adequate levels.
Exercise — The Most Direct Bone-Building Stimulus
Physical activity is the most direct way to stimulate bone formation. Weight-bearing exercise — activity performed on the feet against gravity — puts mechanical stress on bones that directly signals osteoblasts to produce new bone tissue. Walking, jogging, hiking, dancing, tennis, and climbing stairs all qualify as weight-bearing activities. In addition, resistance training — lifting weights or using resistance bands — adds muscle-generated forces to bones that further stimulate density gains.
Balance and coordination exercises — such as tai chi and yoga — do not build bone density directly. However, they significantly reduce fall risk and consequently reduce fracture risk in people whose bones are already fragile. Furthermore, exercise improves muscle strength, posture, and reaction time — all of which reduce the likelihood of falling in the first place. Consequently, a comprehensive exercise programme combines weight-bearing aerobic activity, resistance training, and balance work for maximum bone and fracture prevention benefit.
Bisphosphonate Medications
When lifestyle measures alone are insufficient, medications significantly slow bone loss and in some cases rebuild bone density meaningfully. Bisphosphonates — including alendronate, risedronate, and zoledronic acid — are the most widely prescribed first-line osteoporosis medications. They work by directly inhibiting osteoclast activity, slowing the rate of bone breakdown without affecting osteoblast function.
Alendronate and risedronate are taken orally — weekly or monthly — while zoledronic acid is given as a yearly intravenous infusion. All three significantly reduce the risk of vertebral and hip fractures in clinical trials. Furthermore, once-yearly zoledronic acid is particularly useful for people who find daily or weekly tablet-taking difficult. The most common side effects are gastrointestinal — particularly oesophageal irritation with oral bisphosphonates — which improve with correct administration technique. Consequently, patients should take oral bisphosphonates on an empty stomach with a full glass of water and remain upright for at least 30 minutes afterward.
Anabolic Therapies — Actually Building New Bone
While bisphosphonates slow bone loss, anabolic therapies — drugs that actively stimulate bone formation — go further by building new bone tissue. Teriparatide — a synthetic form of parathyroid hormone — stimulates osteoblast activity directly and produces significant bone density gains at the spine and hip. It is administered as a daily self-injection and is typically reserved for people with severe osteoporosis or those who have fractured despite bisphosphonate therapy.
Romosozumab is the newest anabolic agent. It blocks a protein called sclerostin that normally inhibits osteoblast activity — simultaneously increasing bone formation and decreasing bone breakdown. Clinical trials show that romosozumab produces the most rapid bone density gains of any available osteoporosis medication. Furthermore, it reduces fracture risk significantly within the first year of treatment. However, it requires monthly injections for one year only and is followed by antiresorptive therapy to maintain the gains achieved.
For context on how kidney and autoimmune conditions affect bone health and treatment choices, see our articles on nephrotic syndrome — what protein in the urine actually tells you — and benign prostatic hyperplasia — the enlarged prostate explained.
Prevention of Osteoporosis
Building Strong Bones From Youth
The most effective osteoporosis prevention strategy starts decades before the disease develops. Building the highest possible peak bone mass during childhood, adolescence, and early adulthood provides the largest possible bone reserve to draw on later in life. Adequate calcium and vitamin D throughout growing years, regular physical activity including impact sports, avoidance of smoking, and limited alcohol consumption all maximise peak bone mass.
Furthermore, young women who develop amenorrhoea — the absence of menstrual periods — from low body weight, excessive exercise, or eating disorders experience a significant period of oestrogen deficiency that permanently reduces peak bone mass. Consequently, addressing disordered eating and exercise patterns in young people has lifelong bone health implications that extend far beyond the immediate situation.
Preventing Falls in Older Adults
In people who already have reduced bone density, preventing falls is as important as building bone strength. Home hazard assessment — removing loose rugs, improving lighting, installing grab rails, and clearing walkways — significantly reduces fall risk. Annual vision and hearing checks identify sensory impairments that contribute to balance problems. Moreover, medication review identifies drugs that cause dizziness, sedation, or low blood pressure — all of which increase fall risk in older adults.
Vitamin D supplementation specifically reduces fall risk — in addition to its bone density benefits — by improving muscle function and neuromuscular coordination. Consequently, vitamin D is one of the few interventions that simultaneously reduces both bone fragility and the likelihood of the fall that would trigger a fracture.
When to Seek Medical Help
Speak to a doctor if you are a woman over 65, a man over 70, or a younger person with significant risk factors including steroid use, a history of fragility fracture, early menopause, or a family history of hip fracture. Furthermore, any person who has lost height, developed new back pain, or fractured a bone from minimal trauma needs urgent osteoporosis assessment.
Consequently, do not wait for a fracture to seek evaluation. Early DEXA scanning and FRAX assessment allow treatment to begin before bones reach the fracture threshold — and that early intervention makes the most meaningful difference to long-term bone health and independence.
Frequently Asked Questions
1. Can osteoporosis be completely reversed?
Osteoporosis cannot be fully reversed in most people. However, treatment can significantly slow further bone loss and in some cases meaningfully increase bone density — particularly with anabolic therapies like teriparatide and romosozumab. Furthermore, fracture risk reduces substantially even when bone density gains are modest. Consequently, the goal of treatment is not complete reversal but meaningful fracture risk reduction and preservation of independence and quality of life.
2. Is osteoporosis only a disease of older women?
No. While postmenopausal women face the highest risk, osteoporosis also affects men — particularly after age 70 — and younger people with conditions that cause bone loss, such as coeliac disease, inflammatory bowel disease, early menopause, or long-term corticosteroid use. Furthermore, men are significantly underdiagnosed because osteoporosis is incorrectly perceived as exclusively a women’s health issue. Consequently, any person with significant risk factors deserves bone density assessment regardless of age or sex.
3. How long does osteoporosis treatment take to work?
Bisphosphonates typically show measurable bone density improvements on DEXA scan after one to two years of treatment. Fracture risk reduction, however, begins earlier — within the first year. Anabolic therapies produce faster density gains — often visible within six months. Furthermore, the benefit of treatment continues to accumulate with ongoing use. Consequently, regular DEXA monitoring every one to two years tracks treatment response and guides decisions about continuing, switching, or stopping therapy.
4. Does calcium supplementation alone prevent osteoporosis?
Calcium supplementation alone is not sufficient to prevent or treat osteoporosis. It provides the raw material for bone mineralisation but does not address the imbalance between osteoclast and osteoblast activity that drives bone loss. Furthermore, calcium works most effectively when combined with adequate vitamin D, weight-bearing exercise, and — when indicated — prescription medications. Consequently, a comprehensive approach addressing multiple aspects of bone health simultaneously produces far better outcomes than calcium supplementation in isolation.
5. Can a person with osteoporosis still exercise safely?
Yes, with appropriate guidance. Exercise is not only safe for most people with osteoporosis — it is an essential part of treatment. Weight-bearing and resistance exercises stimulate bone formation and improve muscle strength. However, high-impact activities that risk falling and certain spinal flexion exercises — such as toe touches and sit-ups — may increase fracture risk in people with severe spinal osteoporosis. Consequently, working with a physiotherapist to design a personalised exercise programme tailored to individual bone density and fracture history provides the safest and most effective approach.
References
- Osteosarcoma is the most common primary malignant bone tumor in children and adolescents characterized by malignant osteoblasts producing osteoid and bone.
- Hyperparathyroidism is excessive parathyroid hormone production resulting in elevated serum calcium (hypercalcemia). Classification.
- Primary biliary cholangitis is a chronic autoimmune disease causing progressive inflammation and destruction of intrahepatic bile ducts
Disclaimer
This article adapts publicly available information from WHO’s Osteoporosis page. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform and not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.