
Spondylolisthesis: Slipped Vertebra, Back Pain, and Treatment
The spine is an engineering marvel. Thirty-three individual vertebrae stack precisely on top of each other — held in alignment by ligaments, muscles, and small joints — to create a flexible yet stable column that supports the entire body. However, when one vertebra slips forward out of position relative to the one beneath it, this precise architecture breaks down. The consequences range from mild back pain to severe nerve compression and disability.
Spondylolisthesis is the medical term for this forward slipping of one vertebra over another. The word comes from Greek — spondylos meaning vertebra and listhesis meaning to slip or slide. As a result, the spinal canal narrows, nerve roots become compressed, and the surrounding muscles go into protective spasm. The lower back and legs are most commonly affected.
Spondylolisthesis slipped vertebra back pain treatment is a topic that matters to a wide range of people — from young athletes with stress fractures to older adults with age-related spinal degeneration. Furthermore, many people live with spondylolisthesis for years without knowing it because mild cases produce no symptoms at all. Consequently, understanding what causes vertebrae to slip, how to recognise when slippage is causing harm, and what treatments can restore stability and relieve pain is essential knowledge for anyone dealing with persistent back or leg pain.
Quick Answer
Spondylolisthesis occurs when one vertebra slips forward over the vertebra below it. It causes lower back pain, stiffness, and sometimes leg pain or numbness from nerve compression. It ranges from mild to severe across five grading levels. Treatment starts with physiotherapy and pain management. Surgery stabilises the spine when conservative care fails.
How the Spine Works — and Why Vertebrae Can Slip
The Structure of a Healthy Spinal Segment
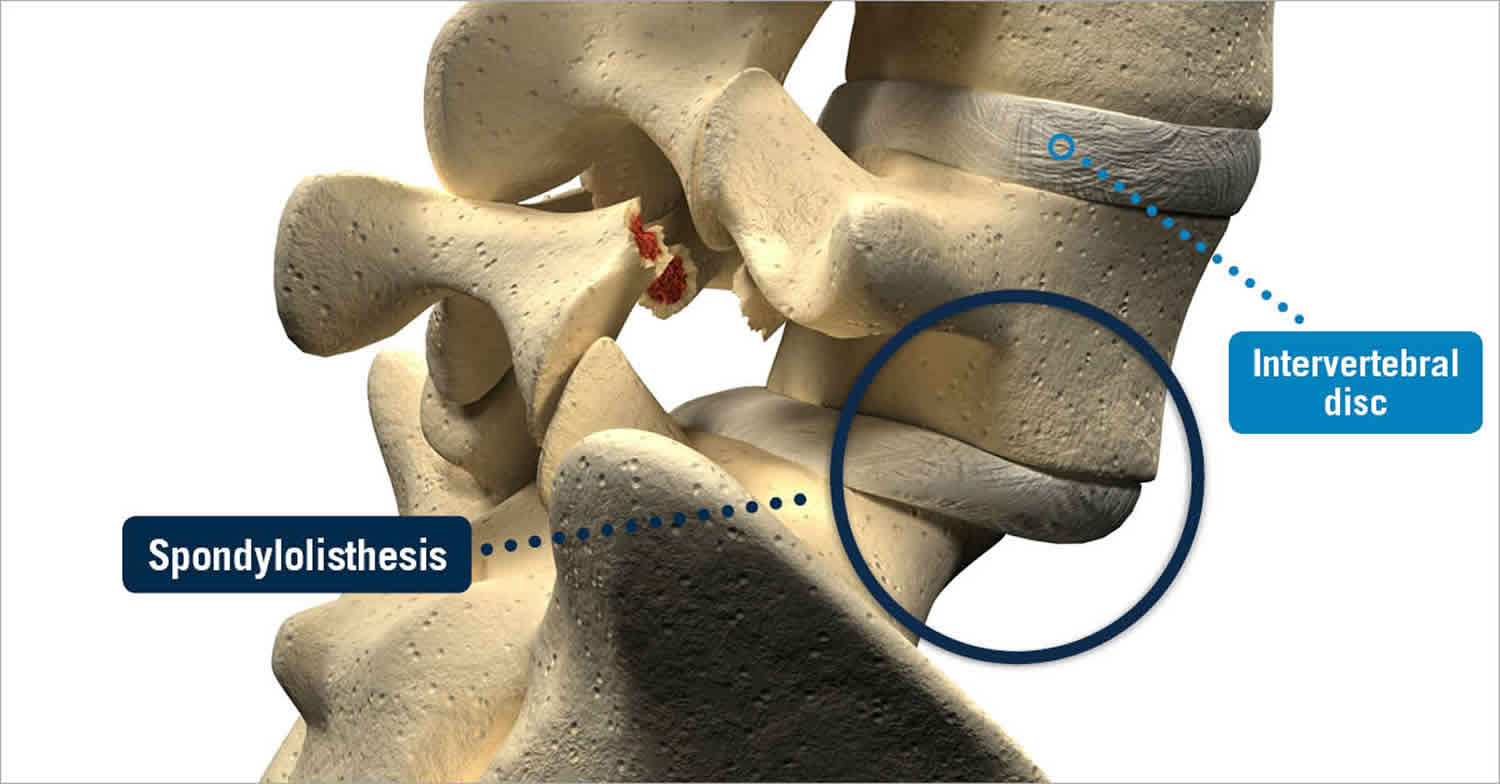
Each spinal segment consists of two vertebrae separated by an intervertebral disc — a cushioning structure that absorbs shock and allows movement. Behind the disc, two small joints called facet joints connect the vertebrae above and below, controlling how far the spine can bend and twist. Furthermore, a bony bridge connecting the upper and lower facet joints on each side — called the pars interarticularis — plays a critical role in preventing forward slippage.
Ligaments and paraspinal muscles provide additional stability across each segment. When all of these structures function normally, the vertebrae remain precisely aligned regardless of the forces placed on the spine during movement, lifting, and physical activity. As a result, the spinal cord and nerve roots running through the spinal canal stay protected and uncompressed.
Why Slippage Occurs
Slippage occurs when the stabilising structures of a spinal segment fail. This failure can result from a stress fracture in the pars interarticularis — removing the bony bridge that prevents forward movement. Alternatively, it can result from degeneration of the disc and facet joints — removing the structural support that keeps the vertebra in position. Furthermore, trauma, abnormal bone development, or weakened bone from conditions such as osteoporosis can all contribute to vertebral instability.
Once a vertebra begins to slip forward, several damaging consequences follow. The disc space narrows asymmetrically. The facet joints on the affected segment experience abnormal stress. The spinal canal and the openings through which nerve roots exit the spine — called neural foramina — narrow progressively. Consequently, nerve roots become compressed, triggering the radiating leg pain, numbness, and weakness that characterise symptomatic spondylolisthesis. For context on how bone density conditions contribute to spinal instability, see our article on osteoporosis — how bones lose density and what reverses it.
Types of Spondylolisthesis
Isthmic Spondylolisthesis
Isthmic spondylolisthesis is the most common type in younger people and athletes. It results from a defect or stress fracture in the pars interarticularis — the narrow bony bridge connecting the upper and lower facet joints. This fracture is called spondylolysis — meaning dissolution of the vertebra — and when it occurs on both sides of the same vertebra, the vertebra loses its bony anchor and slips forward.
Repeated hyperextension — backward bending — of the spine generates the repetitive stress that most commonly causes this fracture. Consequently, isthmic spondylolisthesis is particularly prevalent in young athletes who repeatedly hyperextend their spines — including gymnasts, fast bowlers in cricket, divers, weightlifters, and American football linemen. Furthermore, it most commonly affects the fifth lumbar vertebra — L5 — slipping over the sacrum — S1 — at the base of the spine. In addition, some people are born with a structurally deficient pars interarticularis, making them susceptible to slippage even without significant trauma.
Degenerative Spondylolisthesis
Degenerative spondylolisthesis is the most common type overall and primarily affects adults over 50. It results from age-related degeneration of the intervertebral discs and facet joints — the structures that normally prevent forward slippage. As the disc loses height and the facet joints develop osteoarthritis, the segment becomes unstable. As a result, one vertebra gradually slips forward over time.
Degenerative spondylolisthesis most commonly occurs at the fourth lumbar vertebra — L4 — slipping over L5. Furthermore, it is significantly more common in women than in men — particularly postmenopausal women — and in people with diabetes. The combination of degenerative disc disease and facet joint arthritis produces a pattern where the vertebra slips gradually over months to years. Consequently, symptoms tend to develop insidiously rather than suddenly. For context on how facet joint osteoarthritis contributes to spinal degeneration, see our article on osteoarthritis — inflammation, causes, and what actually helps.
Other Types
Congenital spondylolisthesis — also called dysplastic spondylolisthesis — results from abnormal development of the sacrum or the base of the spine before birth, creating an inherently unstable foundation. Traumatic spondylolisthesis follows acute fractures of the posterior spinal elements other than the pars interarticularis. Pathological spondylolisthesis results from bone weakness caused by conditions including Paget’s disease, tumours, or infection destroying the normal bone architecture. For further context on how bone disease can destabilise spinal structures, see our article on Paget’s disease of bone — deformity, pain, and treatment. Iatrogenic spondylolisthesis develops as a complication of spinal surgery that removes too much of the stabilising posterior bone or joint structures.
Grading of Spondylolisthesis
The Meyerding Classification
Doctors grade spondylolisthesis using the Meyerding classification — a system that divides the degree of slippage into five grades based on the percentage by which the upper vertebra has slipped forward over the lower one.
Grade I represents slippage of up to 25% — typically mild and often asymptomatic. Grade II represents slippage between 26 and 50% — moderate slippage that frequently causes symptoms. Grade III represents slippage between 51 and 75% — severe slippage associated with significant nerve compression and functional limitation. Grade IV represents slippage greater than 75% — very severe instability requiring surgical assessment. Grade V — called spondyloptosis — represents complete slippage where the upper vertebra has fallen entirely off the front of the lower vertebra. This represents the most extreme and surgically complex form of the condition.
Furthermore, the grade at diagnosis does not always predict the rate of future progression. Some Grade I cases remain stable for life. Others progress — particularly in younger patients with active growth or in adults with ongoing degenerative change. Consequently, regular clinical and imaging review is important for all patients with confirmed spondylolisthesis, even those with mild initial grades.
Symptoms of Spondylolisthesis
Lower Back Pain and Stiffness
Spondylolisthesis slipped vertebra back pain treatment is most commonly initiated by lower back pain as the presenting symptom. The pain arises from multiple sources simultaneously — instability of the affected spinal segment, muscle spasm as the paraspinal muscles work harder to compensate for the structural deficit, facet joint inflammation, and disc degeneration at the slipped level.
The pain typically affects the lower back and buttocks. It worsens with prolonged standing, walking, and activities that extend the spine — such as arching backward. Conversely, flexion — bending forward — often temporarily relieves pain by reducing the compressive forces on the posterior spinal structures. Moreover, a characteristic waddle — a side-to-side gait shift — develops in some patients as the body attempts to redistribute weight away from the painful segment. Furthermore, palpating the spine at the level of slippage often reveals a visible or palpable step — a shelf-like depression where the spinous process of the slipped vertebra has moved forward.
Nerve Compression Symptoms
Nerve compression symptoms develop when the slipped vertebra narrows the neural foramen — the opening through which nerve roots exit the spine. Radiculopathy — pain, numbness, or tingling travelling down the leg along the path of the compressed nerve — is a hallmark symptom. L5 nerve root compression — the most commonly compressed level in spondylolisthesis — produces pain and tingling radiating from the buttock down the outside of the thigh and into the top of the foot.
S1 nerve root compression produces pain and tingling down the back of the thigh and into the sole and outside of the foot. Muscle weakness in the affected leg — particularly foot drop from L5 compression — significantly impairs walking and balance. In addition, bowel or bladder dysfunction from severe central canal compression constitutes cauda equina syndrome — a neurological emergency requiring immediate surgical decompression. Consequently, any person with back pain combined with new bladder or bowel problems must seek emergency medical care without delay.
How Doctors Diagnose Spondylolisthesis
Imaging Studies
Diagnosing spondylolisthesis slipped vertebra back pain treatment begins with plain X-ray of the lumbar spine. Standing X-rays — taken in the upright, weight-bearing position — best demonstrate the degree of slippage because gravity increases the forward displacement that may be partially reduced when lying down. Furthermore, lateral — side view — X-rays clearly show the step deformity at the slipped level and measure the degree of slippage as a percentage for Meyerding grading.
Flexion-extension X-rays — taken with the spine bent forward and then arched backward — assess spinal stability by revealing whether the degree of slippage changes with movement. Dynamic instability — where slippage increases significantly with movement — indicates that the segment is mechanically unstable and influences the decision regarding surgical stabilisation. Moreover, the pars interarticularis defect of isthmic spondylolisthesis is often visible on oblique X-ray views as the classic Scotty dog sign — a lucent fracture line across the neck of the dog-shaped bony outline.
MRI scanning provides the most comprehensive assessment of the soft tissue consequences of spondylolisthesis. It directly visualises disc degeneration, facet joint arthritis, nerve root compression, canal stenosis, and any inflammatory changes within the vertebral bodies. Furthermore, MRI identifies the specific nerve roots being compressed — correlating anatomical findings with the patient’s clinical symptoms. Consequently, MRI guides both treatment planning and surgical decision-making with a level of detail that plain X-ray alone cannot provide.
CT scanning adds complementary information about bony anatomy — particularly important when surgical planning requires detailed assessment of bone quality, pedicle size, and the three-dimensional architecture of the slipped segment. In addition, CT myelography — injecting contrast dye into the fluid surrounding the spinal cord — provides excellent nerve root visualisation when MRI is contraindicated.
Clinical Assessment
Clinical assessment begins with a thorough history of pain location, character, and aggravating and relieving factors. Neurological examination assesses leg strength, reflexes, and sensation in the distribution of the potentially compressed nerve roots. Furthermore, straight leg raise testing — lifting the patient’s leg while keeping the knee straight — stretches the sciatic nerve and reproduces radicular pain when nerve root compression is present at L4-5 or L5-S1. Consequently, combining clinical findings with imaging produces the most accurate diagnosis and guides appropriate treatment selection.
Treatment of Spondylolisthesis
Conservative Management
The majority of people with spondylolisthesis — particularly those with Grade I and Grade II slippage — respond well to conservative treatment without surgery. Conservative management aims to reduce pain, strengthen the stabilising muscles around the spine, and prevent further slippage.
Physiotherapy forms the cornerstone of non-surgical treatment. Specific exercise programmes for spondylolisthesis focus on strengthening the core muscles — the deep abdominal and lumbar muscles that provide dynamic stability to the spinal segments. Furthermore, gluteal and hip strengthening reduces the load transferred to the lumbar spine during walking and activity. Hamstring stretching relieves the protective tightness that commonly develops as muscles contract to protect the unstable segment.
Pain management supports participation in physiotherapy by controlling symptoms adequately. Paracetamol and topical NSAIDs provide first-line relief. Oral NSAIDs reduce both pain and the associated muscle spasm. Furthermore, epidural steroid injections — injecting anti-inflammatory medication around the compressed nerve roots — provide targeted relief of radicular leg pain when nerve compression is the dominant symptom. Consequently, a period of structured physiotherapy combined with adequate pain management resolves or significantly improves symptoms in the majority of patients with low-grade spondylolisthesis.
Activity modification — avoiding high-impact spinal loading activities during acute pain phases — protects the unstable segment from progressive stress while healing and strengthening occur. Bracing — using a rigid or semi-rigid lumbar orthosis — is sometimes used in young athletes with active spondylolysis or low-grade isthmic spondylolisthesis to immobilise the defect and promote healing. Moreover, returning to sport and activity should be gradual and guided by symptoms and functional progress rather than by fixed time frames. For context on managing chronic musculoskeletal pain conditions alongside spondylolisthesis, see our article on fibromyalgia — the pain condition that is real, widely misunderstood, and treatable.
Surgical Treatment
Surgery is considered when conservative treatment fails to provide adequate relief after three to six months, when neurological deficits — weakness, numbness, or bowel and bladder dysfunction — are present or worsening, when high-grade slippage threatens spinal stability, or when the quality of life remains severely compromised despite appropriate non-surgical management.
Spinal decompression — removing the bone and ligament tissue pressing on nerve roots — relieves radicular symptoms by widening the compressed neural foramen or spinal canal. However, decompression alone may increase instability in spondylolisthesis. Consequently, decompression is typically combined with spinal fusion in most cases of symptomatic spondylolisthesis requiring surgery.
Spinal fusion permanently connects two adjacent vertebrae — eliminating movement at the unstable segment and preventing further slippage. The surgeon places bone graft material — from the patient’s own iliac crest or from donor bone — between the vertebrae and stabilises the construct with titanium pedicle screws and rods. Over three to twelve months, the bone graft heals and the two vertebrae grow together into a single solid unit. Furthermore, posterior lumbar interbody fusion — called PLIF — and transforaminal lumbar interbody fusion — called TLIF — insert a cage filled with bone graft between the vertebral bodies from behind, restoring disc height and achieving more rigid stabilisation than posterolateral fusion alone.
Minimally invasive spinal fusion techniques — using smaller incisions, specialised retractors, and image guidance — reduce muscle damage, blood loss, and recovery time compared with traditional open surgery. Consequently, minimally invasive TLIF has become the preferred surgical approach in many spinal surgery centres for Grade I and Grade II spondylolisthesis requiring operative stabilisation. For context on how bone quality affects surgical outcomes in spinal conditions, see our article on avascular necrosis — when bone tissue dies from lack of blood supply.
Recovery and Long-Term Outlook
Post-Surgical Rehabilitation
Recovery after spinal fusion surgery requires patience and structured rehabilitation. Most patients return home within two to four days of surgery. However, bone fusion takes three to twelve months to complete. Consequently, heavy lifting, high-impact activity, and significant spinal loading must be avoided until fusion is confirmed on imaging.
Physiotherapy begins within days of surgery — initially focusing on gentle mobilisation, wound care, and preventing post-operative complications. Progressive core strengthening, walking programmes, and functional movement training build the muscle support that protects the fused segment and prevents adjacent segment degeneration over the long term. Furthermore, most patients return to office work within four to six weeks and to manual work within three to six months depending on fusion progress.
Long-Term Management for Non-Surgical Patients
People managing spondylolisthesis conservatively require ongoing attention to core strength, body weight, and activity levels throughout their lives. Regular physiotherapy review ensures that exercise programmes remain appropriate as the condition evolves. Furthermore, maintaining a healthy body weight significantly reduces spinal loading and slows the progression of adjacent disc degeneration that can worsen symptoms over time.
Annual or biennial clinical review — with repeat imaging if symptoms change significantly — monitors for slippage progression and allows timely reassessment of treatment strategy. Moreover, people with confirmed spondylolisthesis should inform any new healthcare provider of their diagnosis before starting any physical treatment or exercise programme that involves spinal loading. Consequently, informed long-term self-management significantly reduces the risk of symptom flares and the need for surgical intervention.
When to Seek Urgent Medical Help
Seek emergency medical care immediately if you develop sudden onset of bowel or bladder dysfunction — inability to urinate, loss of bladder control, or faecal incontinence — alongside lower back pain and leg weakness or numbness. These symptoms may signal cauda equina syndrome — a surgical emergency caused by severe compression of the nerve roots at the base of the spinal canal.
Furthermore, rapidly worsening leg weakness, sudden severe increase in back pain after minor trauma, or new neurological symptoms in a person with known spondylolisthesis all require urgent medical assessment. Consequently, acting immediately when these warning signs appear significantly improves the chance of preventing permanent neurological damage.
Frequently Asked Questions
1. Can spondylolisthesis heal without surgery?
Yes, in many cases. The majority of people with Grade I and Grade II spondylolisthesis manage their condition effectively with physiotherapy, core strengthening, pain management, and activity modification — without ever needing surgery. Furthermore, younger patients with isthmic spondylolysis — the pars fracture that precedes slippage — can sometimes achieve bony healing with immobilisation and rest. Consequently, surgery is reserved for cases where conservative treatment has genuinely failed or where neurological compromise is present.
2. Can spondylolisthesis get worse over time?
Yes, it can progress — though not all cases do. Degenerative spondylolisthesis tends to progress slowly over years as disc and facet joint degeneration continues. Isthmic spondylolisthesis in children and adolescents carries the highest risk of progression during the growth spurt years. Furthermore, high-grade slippage — Grade III or above — carries greater progression risk than low-grade slippage. Consequently, regular imaging monitoring is recommended for all patients with confirmed spondylolisthesis to detect progression before significant neurological compromise develops.
3. Is spondylolisthesis the same as a slipped disc?
No. These are two different spinal conditions. Spondylolisthesis refers to forward slippage of one vertebra over the one below it — a movement of the entire vertebral body. A slipped disc — more accurately called a herniated or prolapsed intervertebral disc — refers to the soft inner material of a spinal disc bulging or rupturing through its outer wall and pressing on adjacent nerve roots. Furthermore, both conditions can cause similar symptoms including back and leg pain. Consequently, accurate imaging is essential to distinguish between them and choose the correct treatment.
4. Can young children develop spondylolisthesis?
Yes. Isthmic spondylolisthesis can develop in children — particularly active children involved in sports that stress the lumbar spine through repeated hyperextension. It is most commonly identified between the ages of 8 and 14, often during the adolescent growth spurt when rapid bone growth temporarily outpaces the strength of the bony pars interarticularis. Furthermore, congenital spondylolisthesis — resulting from abnormal spinal development before birth — can also present in childhood. Consequently, persistent low back pain in a young athlete — particularly after hyperextension activities — warrants imaging assessment for spondylolysis or spondylolisthesis.
5. What is the difference between spondylolysis and spondylolisthesis?
Spondylolysis refers specifically to a stress fracture or defect in the pars interarticularis — the bony bridge connecting the facet joints — without any forward slippage of the vertebra. It is the precursor condition to isthmic spondylolisthesis. Spondylolisthesis occurs when spondylolysis is bilateral — present on both sides of the same vertebra — and the vertebra subsequently slips forward. Furthermore, spondylolysis can exist without progressing to spondylolisthesis — particularly in adults — though it still causes significant back pain requiring treatment. Consequently, both conditions require imaging for accurate diagnosis and distinction from each other.
Conclusion
Spondylolisthesis is a common spinal condition that ranges from a mild, incidentally discovered finding to a severely disabling disorder with nerve compression and significant functional limitation. When a vertebra slips out of position — whether from a stress fracture, degenerative change, or structural weakness — the effects on the spine, nerves, and quality of life can be profound.
Spondylolisthesis slipped vertebra back pain treatment has advanced significantly — from simple rest and pain relief to targeted physiotherapy, minimally invasive surgery, and precise fusion techniques that restore spinal stability with excellent long-term outcomes. Furthermore, the majority of patients with low-grade disease achieve satisfactory symptom control without surgery when they engage consistently with core strengthening and structured rehabilitation.
If you experience persistent lower back pain, radiating leg pain, or any of the warning signs described in this article — particularly new bowel or bladder symptoms — seek medical attention promptly. Consequently, early diagnosis, accurate grading, and timely treatment give people with spondylolisthesis the best possible chance of living actively, comfortably, and well for years to come.
References
- Ankylosing spondylitis is a chronic autoimmune inflammatory arthritis primarily affecting the spine and sacroiliac joints.
- Indian batting coach Sitanshu Kotak shared his thoughts on the implications of the slope during a recent press conference.
This article adapts publicly available information from WHO’s Musculoskeletal Conditions page. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform and not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.