
Septic Arthritis: The Joint Infection That Destroys Cartilage
Most joint conditions develop slowly. Osteoarthritis progresses over years. Inflammatory arthritis builds over weeks to months. However, septic arthritis works on an entirely different and far more dangerous timescale. It can destroy the cartilage of a joint within days — and without emergency treatment, the damage becomes permanent.
Septic arthritis is a joint infection caused by bacteria — or, less commonly, viruses or fungi — that invade the joint space directly. Once inside the joint, bacteria multiply rapidly and trigger an intense inflammatory response. Proteolytic enzymes — protein-dissolving chemicals released by bacteria and immune cells — attack and destroy cartilage with devastating speed. The result is irreversible joint destruction that no amount of later treatment can fully repair.
Septic arthritis joint infection destroys cartilage through a mechanism that operates over days rather than years. Furthermore, it carries a mortality rate of up to 15% even in well-resourced healthcare settings when diagnosis is delayed. Consequently, recognising septic arthritis quickly — and distinguishing it from other causes of acute joint pain — is one of the most important skills in urgent clinical medicine. This article explains what causes it, how it presents, and why the window for saving a joint is measured in hours rather than weeks.
Quick Answer
Septic arthritis is a bacterial joint infection that triggers intense inflammation and rapid cartilage destruction within days. It causes a single acutely hot, swollen, and exquisitely painful joint — often with fever. It constitutes a medical emergency requiring immediate joint drainage and intravenous antibiotics. Delayed treatment leads to permanent joint destruction and life-threatening sepsis.
How Septic Arthritis Destroys Cartilage
The Speed of Bacterial Damage
Understanding why septic arthritis joint infection destroys cartilage so rapidly requires a picture of what happens inside an infected joint. Bacteria entering the joint space encounter a warm, nutrient-rich environment with limited immune surveillance. They multiply exponentially — doubling in number every twenty to thirty minutes under ideal conditions. Within hours, the bacterial load inside the joint reaches levels that trigger an overwhelming immune response.
Neutrophils — the immune system’s frontline defensive cells — flood into the joint space in enormous numbers. They release proteolytic enzymes — chemicals that break down proteins — including matrix metalloproteinases and serine proteases. These enzymes target collagen and proteoglycans — the structural components of cartilage. Furthermore, bacteria themselves produce toxins that directly damage cartilage cells called chondrocytes.
Why Cartilage Cannot Recover
Cartilage has a critically limited capacity for self-repair. It contains no blood vessels — meaning it relies entirely on the slow diffusion of nutrients through synovial fluid for its maintenance. Consequently, when the synovial environment becomes toxic with bacterial products, inflammatory chemicals, and enzymatic debris, cartilage cells die and the matrix they maintain dissolves rapidly.
The subchondral bone — the bone directly beneath the cartilage — quickly becomes involved as infection spreads from the joint space. Osteomyelitis — bone infection — develops within days in untreated cases. Furthermore, the joint capsule and surrounding soft tissues become infiltrated with infection. Consequently, the window for preserving joint function narrows with every hour of diagnostic delay — making septic arthritis one of the few true emergencies in musculoskeletal medicine.
What Causes Septic Arthritis?
Bacterial Routes Into the Joint
Bacteria reach the joint space through three main pathways. Haematogenous spread — bacteria travelling through the bloodstream from an infection elsewhere in the body — is the most common route. Any bacterial infection producing bacteraemia — bacteria in the bloodstream — can seed a joint. Common sources include skin infections, urinary tract infections, intravenous drug use sites, dental procedures, and infected catheters or lines.
Direct inoculation occurs when bacteria are introduced directly into the joint through a penetrating injury, a joint injection, joint aspiration, or arthroscopic surgery. Furthermore, wound infections following orthopaedic procedures — including joint replacement surgery — represent an increasingly important cause of septic arthritis. Consequently, any patient who develops acute joint pain and swelling in the weeks following joint surgery requires urgent assessment to exclude prosthetic joint infection.
Contiguous spread — bacteria spreading from an adjacent focus of osteomyelitis or soft tissue infection directly into the joint space — is the third pathway. This route is particularly important in children, where the blood supply anatomy of the growing skeleton places bone metaphyses — the growing ends of bones — immediately adjacent to joint spaces. Consequently, osteomyelitis in children frequently extends directly into the adjacent joint.
The Most Common Bacteria
Staphylococcus aureus is the most common causative organism of septic arthritis across all age groups. It is a particularly aggressive pathogen — producing toxins that accelerate cartilage destruction and forming biofilms on joint surfaces that make eradication with antibiotics alone extremely difficult. Furthermore, methicillin-resistant Staphylococcus aureus — called MRSA — presents additional treatment challenges because it resists standard antibiotic regimens.
Streptococcal species — including Streptococcus pyogenes and Streptococcus pneumoniae — are the second most common group of causative organisms. In sexually active young adults, Neisseria gonorrhoeae — the bacterium causing gonorrhoea — is an important cause of septic arthritis and produces a distinctive clinical syndrome including migratory arthritis, skin lesions, and tenosynovitis before settling in a single joint.
In children under two years of age, Haemophilus influenzae was historically an important pathogen — though routine vaccination has dramatically reduced its prevalence. In older adults and immunocompromised patients, gram-negative organisms including Escherichia coli and Pseudomonas aeruginosa cause a significant proportion of cases. Consequently, antibiotic choice must account for likely organism based on patient age, risk factors, and local resistance patterns.
Who Is Most at Risk?
Several factors dramatically increase the risk of septic arthritis. Pre-existing joint disease — particularly rheumatoid arthritis — significantly elevates risk because inflamed synovium is more vulnerable to bacterial seeding. Furthermore, prosthetic joints — artificial hip and knee replacements — are highly susceptible to infection because bacteria adhere readily to metal and plastic surfaces and form biofilms that resist antibiotic penetration.
Immunocompromised states — including diabetes mellitus, HIV infection, malignancy, organ transplantation, and immunosuppressive medication — impair the body’s ability to contain bacteraemia before it seeds a joint. Intravenous drug use provides direct and repeated routes for bacteria to enter the bloodstream. Moreover, skin conditions causing breaks in the protective barrier — including eczema, psoriasis, and chronic ulceration — create portals for bacterial entry. Consequently, any patient with acute monoarthritis — inflammation of a single joint — and one or more of these risk factors demands urgent septic arthritis assessment. For context on how immunosuppressive conditions increase infection risk, see our article on lupus nephritis — when lupus attacks the kidneys.
Symptoms of Septic Arthritis
The Acute Presentation
Septic arthritis joint infection destroys cartilage silently in its earliest hours — before symptoms become dramatic. However, symptoms typically escalate rapidly over twelve to twenty-four hours. The affected joint becomes acutely painful — with a severity that patients consistently describe as unlike any pain they have experienced before. Movement of the joint in any direction dramatically worsens the pain. Consequently, the person with septic arthritis characteristically holds the joint completely still in a position of maximum comfort — typically slight flexion.
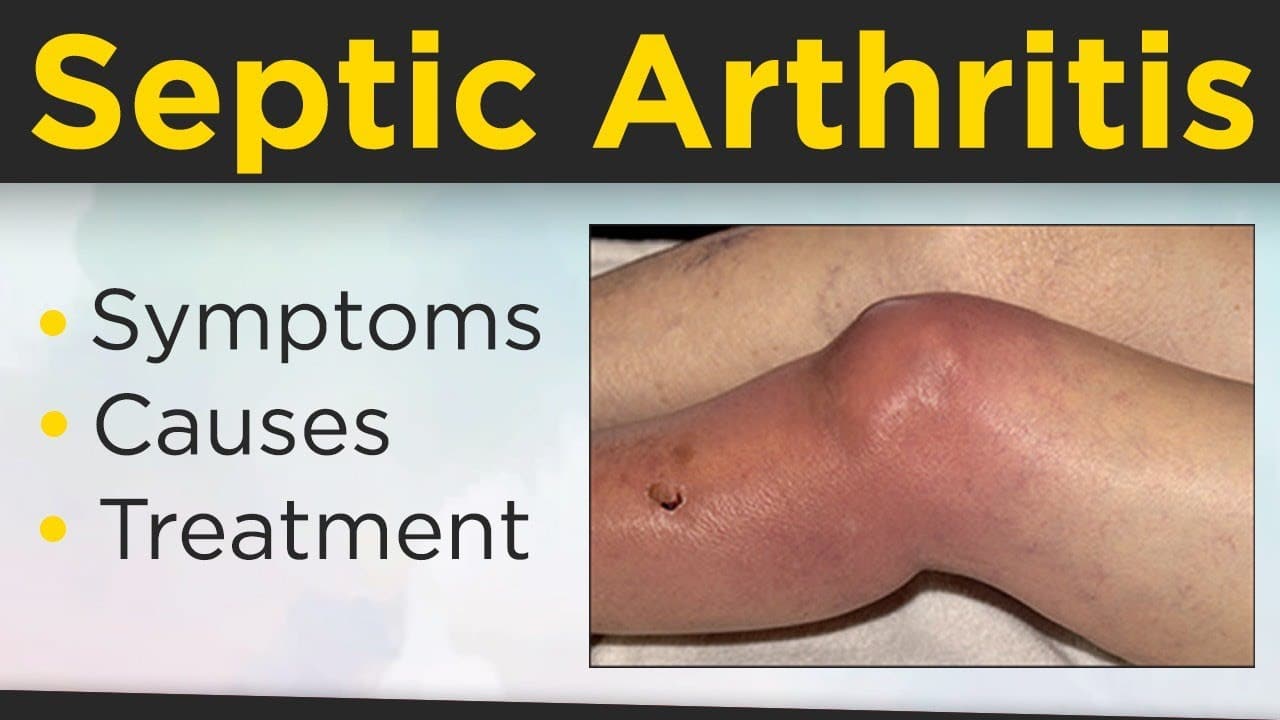
The joint swells visibly as bacteria-laden inflammatory fluid rapidly accumulates in the joint space. The overlying skin becomes warm and red as the intense local inflammation increases blood flow to the area. Furthermore, fever — typically above 38.5 degrees Celsius — and systemic illness develop as the infection triggers a whole-body inflammatory response. The person feels acutely unwell — not merely uncomfortable.
The Most Commonly Affected Joints
Any joint can develop septic arthritis. However, the knee is the most commonly affected joint in adults — accounting for roughly 50% of all cases. The hip is the second most commonly affected and presents particular diagnostic challenges because deep anatomical location makes the classical signs of warmth and swelling less obvious on external examination. Furthermore, hip septic arthritis in children may initially appear as reluctance to bear weight or limp rather than obvious joint swelling.
Other commonly affected joints include the shoulder, wrist, ankle, and sacroiliac joints. Polyarticular septic arthritis — infection of multiple joints simultaneously — occurs in roughly 15 to 20% of cases — particularly in patients with rheumatoid arthritis or disseminated gonococcal infection. Moreover, spinal septic arthritis — called septic discitis or vertebral osteomyelitis — produces a different clinical picture including severe back pain and fever without obvious peripheral joint swelling. Consequently, septic arthritis presents across a wide spectrum of severity and joint distribution.
How Doctors Diagnose Septic Arthritis
The Critical Importance of Joint Aspiration
No investigation is more important in suspected septic arthritis than joint aspiration — withdrawing synovial fluid from the joint with a needle. Doctors perform this at the bedside or under ultrasound guidance and must not delay it waiting for imaging results or specialist review when clinical suspicion is high.
Joint fluid analysis provides the most directly useful information available. In septic arthritis, the fluid is typically turbid — cloudy — with a markedly elevated white cell count — usually above 50,000 cells per microlitre, frequently above 100,000. Furthermore, the fluid Gram stain — a rapid microscopy technique that stains bacteria — identifies the causative organism in roughly 50 to 75% of bacterial cases within minutes of aspiration. Fluid culture — growing the organism in a laboratory — takes twenty-four to seventy-two hours but provides definitive organism identification and antibiotic sensitivity data. Consequently, aspiration both establishes the diagnosis and guides antibiotic selection simultaneously.
Blood Tests and Imaging
Blood tests support the diagnosis and assess disease severity. The white blood cell count, CRP — C-reactive protein — and ESR — erythrocyte sedimentation rate — are typically markedly elevated. Blood cultures — taking blood samples to detect bacteria in the bloodstream — identify the causative organism in roughly 25 to 50% of cases and must be taken before antibiotics are started. Furthermore, blood lactate levels reflect the severity of systemic inflammatory response and help identify patients at risk of rapid deterioration toward septic shock.
Plain X-ray of the affected joint is usually normal in early septic arthritis — the bony and cartilaginous destruction that X-ray detects takes days to weeks to develop. However, X-ray excludes other urgent diagnoses including fracture and identifies pre-existing joint disease. Ultrasound rapidly and reliably detects joint effusion — particularly in the hip where clinical examination is unreliable — and guides aspiration of deep joints. MRI provides the most sensitive assessment of early bone involvement and soft tissue extension of infection. Consequently, MRI is particularly valuable when osteomyelitis is suspected alongside joint infection.
Treatment of Septic Arthritis
Emergency Joint Drainage
Septic arthritis is a surgical emergency. Joint drainage — removing the infected fluid from the joint — is the single most important treatment step and must not wait for microbiology results. The infected fluid contains billions of bacteria, proteolytic enzymes, and inflammatory debris. Every hour it remains in the joint accelerates irreversible cartilage destruction.
Repeated needle aspiration — withdrawing fluid through a needle once or twice daily — achieves adequate drainage in many cases, particularly for accessible joints such as the knee. This approach avoids the risks and recovery associated with surgery. However, it requires daily clinical review and repeat aspiration as long as fluid continues to reaccumulate. Furthermore, if fluid recurs rapidly despite daily aspiration, or if the joint fails to improve clinically within forty-eight to seventy-two hours, surgical drainage becomes necessary.
Surgical Drainage Options
Arthroscopic washout — flushing the joint with large volumes of sterile saline using a keyhole camera and instruments — removes infected material more thoroughly than needle aspiration and allows direct visualisation of cartilage damage. It is the preferred surgical approach for most joints because it combines thorough lavage with minimal surgical trauma. Furthermore, arthroscopy allows removal of necrotic tissue and fibrin deposits that harbour bacteria and impair healing.
Open surgical drainage — making a formal incision to directly access the joint — is reserved for joints where arthroscopy is technically challenging — particularly the hip in children — for cases with extensive soft tissue involvement, and for prosthetic joint infections requiring implant removal. Moreover, prosthetic joint infection management follows a distinct protocol — typically involving removal of the implant, prolonged antibiotic therapy, and staged reimplantation — because bacteria embedded in biofilm on the prosthesis resist antibiotic penetration entirely. Consequently, orthopaedic surgeon involvement is essential for all cases of prosthetic joint infection from the moment of diagnosis.
Intravenous Antibiotic Therapy
Intravenous antibiotics must start immediately after blood cultures and joint aspiration are completed — without waiting for culture results. Empirical antibiotic choice covers the most likely organisms based on patient age, risk factors, and local resistance patterns. In most adults, empirical therapy targets Staphylococcus aureus and Streptococcal species — typically using flucloxacillin in settings with low MRSA prevalence or vancomycin where MRSA is a significant risk.
Antibiotics are then adjusted within twenty-four to seventy-two hours once culture and sensitivity results confirm the causative organism and its antibiotic susceptibility profile. Intravenous therapy continues for a minimum of two weeks in most cases — longer when osteomyelitis accompanies joint infection. Furthermore, transition to oral antibiotic therapy after clinical improvement and falling inflammatory markers is now standard practice in many centres — supported by evidence from clinical trials showing equivalence between prolonged intravenous and sequential oral therapy in selected patients. Consequently, the total antibiotic course for septic arthritis typically ranges from four to six weeks depending on the causative organism and clinical response.
Rehabilitation After Septic Arthritis
Physiotherapy begins as soon as the acute infection is controlled — typically within the first few days of treatment. Early gentle joint movement maintains cartilage nutrition through synovial fluid circulation and prevents the adhesions and stiffness that develop rapidly after joint infection.
Progressive range of movement and strengthening exercises restore function as inflammation subsides. Furthermore, weight-bearing on lower limb joints resumes gradually — guided by pain, swelling reduction, and inflammatory marker trends. Consequently, the rehabilitation timeline after septic arthritis varies considerably — from two to four weeks for cases treated promptly with minimal cartilage damage to several months for cases with significant joint destruction or concurrent osteomyelitis. For context on how inflammatory joint conditions respond to physiotherapy and long-term management, see our article on reactive arthritis — when infection triggers joint pain.
Long-Term Outcomes and Monitoring
When Treatment Succeeds
The long-term outcome of septic arthritis depends critically on how quickly treatment begins. When joint drainage and antibiotics start within twenty-four hours of symptom onset, the majority of patients recover good joint function without permanent damage. Furthermore, outcomes are significantly better in younger patients with no pre-existing joint disease and in cases caused by less virulent organisms.
However, even with optimal treatment, some degree of cartilage damage occurs in a significant proportion of cases. Residual stiffness, reduced range of movement, and secondary osteoarthritis are common sequelae — particularly when the knee or hip has been affected. Consequently, long-term physiotherapy and rheumatology follow-up are important for monitoring joint function recovery and detecting the early development of post-infectious arthritis. For context on how post-infectious joint damage progresses to osteoarthritis, see our article on osteoarthritis — inflammation, causes, and what actually helps.
When Joint Destruction Occurs
When treatment is delayed beyond forty-eight to seventy-two hours — or when the causative organism is particularly virulent — significant and irreversible cartilage destruction occurs. The joint space narrows progressively on serial X-rays. Bone destruction and erosion become visible. Fibrous adhesions form within the joint cavity.
In severe cases, the joint loses all useful movement — a condition called fibrous ankylosis — requiring eventual joint replacement surgery to restore function. Furthermore, adjacent osteomyelitis complicates recovery significantly — requiring prolonged antibiotic therapy and sometimes surgical bone debridement before the infection fully clears. Consequently, patients with delayed diagnosis face a substantially different — and far more challenging — recovery trajectory than those diagnosed and treated within the critical early window.
When to Seek Emergency Medical Help
Go to an emergency department immediately if any joint becomes acutely hot, severely swollen, and exquisitely tender — particularly if accompanied by fever, shaking chills, or feeling systemically unwell. Do not wait. Do not take anti-inflammatory medications before seeking assessment — they can partially mask the fever and clinical signs and delay diagnosis.
Furthermore, any person with a joint replacement who develops new pain, swelling, or warmth around the implant needs urgent orthopaedic assessment for prosthetic joint infection — even without fever. Consequently, the rule for all clinicians and patients is simple — an acute hot swollen joint is septic arthritis until proven otherwise, and the proof requires joint aspiration, not watchful waiting.
Frequently Asked Questions
1. How quickly does septic arthritis damage a joint?
Cartilage destruction begins within hours of bacterial invasion of the joint space. Significant and potentially irreversible damage can occur within twenty-four to forty-eight hours of symptom onset without treatment. Furthermore, the rate of destruction depends on the virulence of the causative organism — Staphylococcus aureus produces joint destruction more rapidly than most other bacteria. Consequently, every hour of delay between symptom onset and joint drainage and antibiotic treatment directly increases the extent of permanent joint damage.
2. How is septic arthritis different from reactive arthritis?
Septic arthritis involves live bacteria physically present and multiplying inside the joint space — causing direct tissue destruction. Reactive arthritis involves no bacteria inside the joint — instead, the immune system’s response to an infection elsewhere triggers joint inflammation indirectly. Furthermore, septic arthritis is a life-threatening emergency requiring immediate drainage and antibiotics. Reactive arthritis is managed with anti-inflammatory medications and typically resolves without joint drainage. Consequently, distinguishing between them through joint aspiration and fluid culture is clinically essential. For more on reactive arthritis, see our article on reactive arthritis — when infection triggers joint pain.
3. Can septic arthritis occur in a prosthetic joint?
Yes. Prosthetic joint infection — septic arthritis in a joint replacement — is a devastating complication of hip and knee replacement surgery. It affects roughly 1 to 2% of primary joint replacements. Furthermore, bacteria form biofilms on the implant surface that antibiotics cannot penetrate — meaning cure almost always requires surgical removal of the implant. Consequently, any pain, swelling, or redness around a joint replacement — even months or years after surgery — requires urgent orthopaedic assessment to exclude prosthetic joint infection.
4. Can septic arthritis be prevented?
Complete prevention is not always possible. However, several measures significantly reduce risk. Treating bacterial infections promptly before they produce bacteraemia reduces the chance of joint seeding. Meticulous sterile technique during joint injections and arthroscopic procedures minimises direct inoculation risk. Furthermore, prophylactic antibiotics before dental procedures are recommended for patients with prosthetic joints in some guidelines. Consequently, people with prosthetic joints, rheumatoid arthritis, or other high-risk conditions should discuss preventive strategies with their healthcare team. For context on how conditions like chronic kidney disease and diabetes increase infection risk, see our article on chronic kidney disease — stages, symptoms, and how to slow the decline.
5. Does septic arthritis always require surgery?
No. Many cases of septic arthritis in accessible joints — particularly the knee — respond adequately to repeated needle aspiration combined with intravenous antibiotics without formal surgery. However, surgery becomes necessary when repeated aspiration fails to control the infection, when the joint is deep and difficult to aspirate reliably — such as the hip — when osteomyelitis accompanies the infection, or when a prosthetic joint is involved. Consequently, the decision between repeated aspiration and surgical drainage requires daily clinical reassessment rather than a single fixed treatment plan determined at initial presentation.
Conclusion
Septic arthritis is one of the few true emergencies in musculoskeletal medicine. It destroys joint cartilage within days, produces life-threatening sepsis when untreated, and leaves permanent disability when treatment is delayed beyond the narrow critical window. Every hour matters from the moment symptoms begin.
Septic arthritis joint infection destroys cartilage through a relentless cascade of bacterial multiplication, enzymatic tissue destruction, and immune-mediated inflammation that waits for no one. Furthermore, recognising the hallmark clinical pattern — a single acutely hot, swollen, exquisitely painful joint with fever — and acting on it with immediate joint aspiration and intravenous antibiotics is the difference between a saved joint and a destroyed one.
If you or someone near you develops sudden, severe pain in a single joint — particularly with fever and feeling systemically unwell — treat it as a medical emergency and go directly to a hospital. Consequently, acting within hours rather than days gives the joint its only real chance of surviving septic arthritis intact.
References
- The mechanism is brutal. When infection strikes, the immune system floods the bloodstream with chemicals to fight it.
- Rheumatoid arthritis is a chronic autoimmune disease where the body’s immune system mistakenly attacks the synovial lining of joints
- Psoriatic arthritis is a chronic autoimmune inflammatory disease where the immune system attacks joint linings and surrounding tissues in people with psoriasis.
- Reactive arthritis is exactly this phenomenon. It is a form of inflammatory arthritis that develops as the immune system’s response to an infection elsewhere in the body.
Disclaimer
This article adapts publicly available information from WHO’s Musculoskeletal Conditions page. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform and not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.