
Plantar Fasciitis: Why Your Heel Hurts and How to Fix It
That stabbing pain in the heel with the very first step of the morning — sharp, intense, and completely unwelcome — is one of the most recognisable symptoms in all of musculoskeletal medicine. It fades after a few minutes of walking. Then it returns again after sitting for a long time. Millions of people live with this pattern every single day.
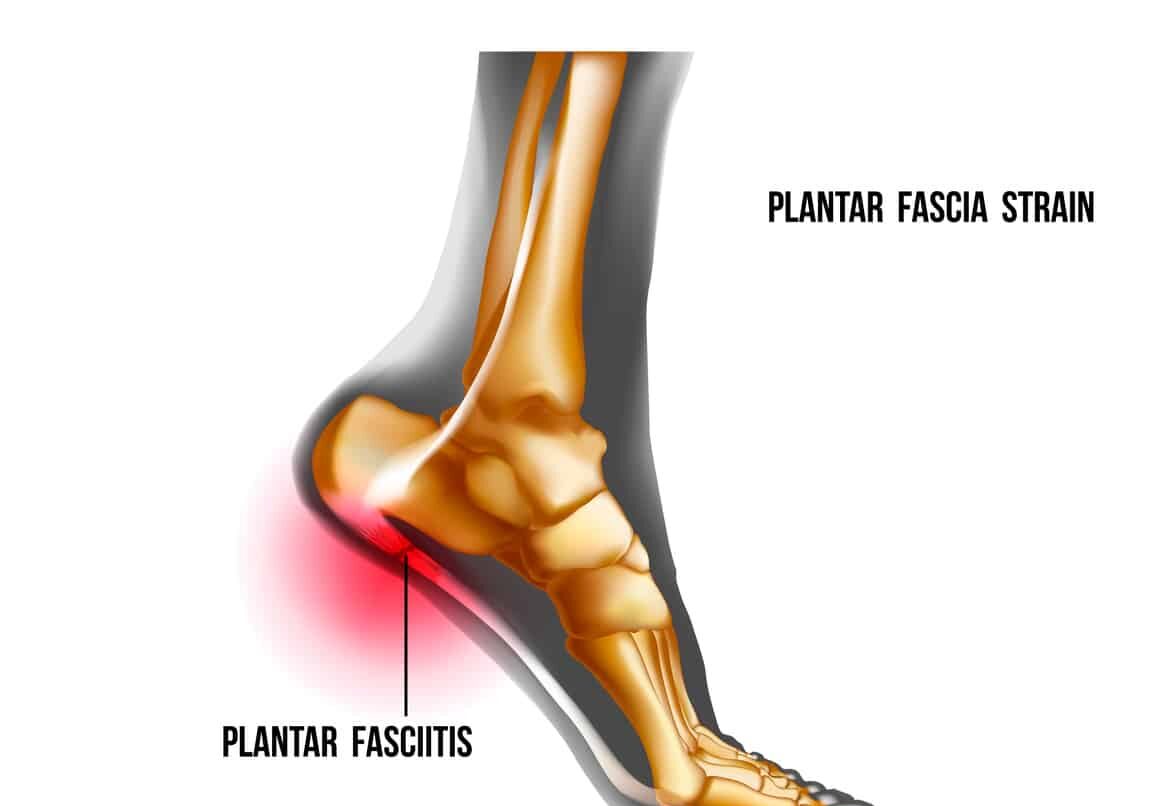
Plantar fasciitis is the most common cause of heel pain worldwide. It affects the plantar fascia — a thick band of connective tissue running along the sole of the foot from the heel bone to the toes. When this band becomes irritated, inflamed, and overloaded, it produces the characteristic sharp heel pain that makes those first morning steps so distinctly unpleasant.
Plantar fasciitis heel pain morning fix is the central theme of this article. Furthermore, this condition affects people of all ages and activity levels — from professional runners to office workers who spend long hours standing on hard floors. Consequently, understanding why the heel hurts in the morning, what makes it worse, and what genuinely fixes it gives patients the tools they need to recover faster and prevent the pain from returning.
Quick Answer
Plantar fasciitis causes sharp heel pain — worst in the morning — because the plantar fascia tightens during sleep and is suddenly stretched with the first steps of the day. Causes include tight calf muscles, flat feet, obesity, and prolonged standing. Treatment combines stretching exercises, footwear changes, and targeted therapies that work well for most people.
What Is the Plantar Fascia?
Anatomy and Function
The plantar fascia is a broad, flat band of fibrous connective tissue. It runs along the bottom of the foot from the heel bone — called the calcaneus — forward to the base of the toes. Think of it as a thick elastic bowstring that supports the arch of the foot and absorbs the shock of every step.
With each step, the plantar fascia stretches as the foot bears weight. When the heel lifts during the push-off phase of walking, the fascia tightens further. Consequently, this tissue experiences enormous cumulative stress over thousands of steps each day. Furthermore, it must manage both the compressive forces of body weight and the tensile forces of the calf muscles pulling through the Achilles tendon above.
Why It Becomes Painful
In plantar fasciitis, repeated microtrauma — tiny injuries from excessive loading — accumulates in the fascia faster than the tissue can repair itself. The result is a degenerative process within the collagen fibres of the fascia near its attachment to the heel bone. Inflammation develops around the damaged tissue. Consequently, the heel becomes painful, particularly when the fascia is placed under sudden load after a period of rest.
The term plantar fasciitis — meaning inflammation of the plantar fascia — is actually somewhat misleading. Research shows that chronic cases involve more degeneration than active inflammation. Nevertheless, the inflammatory phase is important in early disease. Moreover, both phases respond well to treatment when addressed correctly and promptly.
Why Does It Hurt Most in the Morning?
What Happens During Sleep
The characteristic morning heel pain of plantar fasciitis has a clear biological explanation. During sleep, the foot naturally rests in a plantarflexed position — toes pointing downward with the ankle relaxed. In this position, the plantar fascia shortens and tightens over several hours.
Furthermore, the body attempts minor repair of the microtrauma in the fascia overnight. This repair process involves inflammatory activity and slight scar tissue deposition within the damaged fibres. Consequently, the fascia becomes stiffer and more contracted by morning than it was at the end of the previous day.
The First Step Mechanism
When a person places their foot on the floor with that first morning step, the plantar fascia is suddenly and forcefully stretched from its overnight shortened position. This abrupt lengthening tears through the fragile overnight repair tissue and triggers an acute inflammatory response. The result is that sharp, stabbing heel pain that sufferers describe so consistently.
After several minutes of walking, the fascia warms up and gradually lengthens. The acute pain typically diminishes. However, after sitting at a desk or in a car for an extended period, the fascia shortens again — and the pain returns on standing. This pattern of pain after rest — called post-static dyskinesia — is one of the most diagnostically reliable features of plantar fasciitis. For context on other conditions where morning stiffness and pain after rest are key diagnostic features, see our article on osteoarthritis — inflammation, causes, and what actually helps.
Causes and Risk Factors
Biomechanical Causes
Plantar fasciitis heel pain morning fix begins with understanding its causes. Several biomechanical factors increase the load on the plantar fascia beyond its tolerance threshold. Tight calf muscles — particularly the gastrocnemius and soleus — restrict ankle dorsiflexion — the ability to bend the foot upward. When dorsiflexion is restricted, the foot compensates by pronating excessively — rolling inward during each step. This excessive pronation increases the tensile stress on the plantar fascia with every stride.
Flat feet — called pes planus — reduce the arch that the plantar fascia supports. As a result, the fascia is held in a chronically stretched and stressed position throughout standing and walking. In contrast, high arches — called pes cavus — concentrate load in a smaller area of the fascia and can also predispose to plantar fasciitis. Consequently, both extremes of arch height increase plantar fascia vulnerability through different mechanical mechanisms.
Lifestyle and Load Factors
Obesity significantly increases plantar fasciitis risk. Every extra kilogram of body weight adds directly to the compressive and tensile forces on the plantar fascia with every step. Furthermore, a sudden increase in activity level — starting a new running programme, significantly increasing step count, or beginning a job involving prolonged standing — overloads the fascia before it has adapted to the new demands.
Occupations requiring prolonged standing on hard floors — including nursing, teaching, retail, and construction — generate cumulative fatigue in the plantar fascia that exceeds its repair capacity over time. Moreover, footwear plays a critical role. Walking barefoot on hard surfaces, wearing worn-out shoes with inadequate arch support, or transitioning suddenly to minimalist footwear all reduce the shock absorption and arch support the plantar fascia depends on. Consequently, footwear assessment forms an essential component of any plantar fasciitis management plan.
Age and Training Errors
Age increases plantar fasciitis risk because tendon and fascia tissue loses elasticity and blood supply with advancing years. The condition most commonly affects adults between 40 and 60. However, it also affects younger athletes — particularly runners — who rapidly increase their training load, change running surface, or neglect calf and foot flexibility.
Running errors including increasing weekly mileage too quickly, adding hill training, and transitioning between shoe types all represent common precipitants in athletic populations. Furthermore, inadequate warm-up and cool-down routines allow the plantar fascia to remain chronically shortened and unready for the stresses of training. Consequently, training load management is as important as footwear and flexibility in preventing plantar fasciitis in active people. For context on how bone density and foot health interact in older adults, see our article on osteoporosis — how bones lose density and what reverses it.
Symptoms of Plantar Fasciitis
The Classic Pain Pattern
Plantar fasciitis heel pain morning fix relies on recognising its characteristic symptom pattern. Pain at the heel — specifically at the medial tubercle of the calcaneus, the bony bump on the inner side of the heel — is the defining symptom. It strikes sharply with the first steps of the morning or after any period of prolonged rest.
The pain is often described as a stabbing, burning, or aching sensation deep within the heel. Furthermore, it may radiate along the arch toward the toes in some patients. The severity varies from a dull ache to severe pain that significantly limits walking. Consequently, untreated plantar fasciitis progressively impairs the ability to walk comfortably for any sustained distance.
What Makes It Better and Worse
The post-static dyskinesia pattern — pain after rest that improves with movement — is the most diagnostically reliable feature. Pain typically eases after the first five to ten minutes of walking as the fascia warms and lengthens. However, it returns after extended standing or walking, particularly toward the end of a working day.
Stair climbing — particularly ascending stairs on the toes — reproduces the pain reliably because it maximally loads the plantar fascia. Furthermore, walking barefoot on hard surfaces or in flat, unsupportive footwear typically worsens symptoms. In contrast, wearing shoes with firm arch support and a slight heel raise generally reduces pain during activity. Consequently, symptom response to footwear changes provides both diagnostic and therapeutic information simultaneously.
When Symptoms Suggest Something Else
Most heel pain in adults represents plantar fasciitis. However, several other conditions produce heel pain that mimics the plantar fasciitis pattern and require different treatment. Heel stress fractures cause localised bony tenderness and worsen with activity rather than improving after initial warm-up. Tarsal tunnel syndrome — compression of the tibial nerve as it passes around the inner ankle — produces burning, tingling, and numbness along the sole rather than localised heel pain.
Fat pad atrophy — thinning of the protective fat pad beneath the heel — produces diffuse heel pain without a clearly localised tender spot. Moreover, nerve entrapment of the medial calcaneal nerve produces heel pain with a burning quality. Consequently, any heel pain that fails to follow the classic post-static dyskinesia pattern, or that does not respond to standard plantar fasciitis treatment, deserves specialist reassessment to exclude these alternative diagnoses.
How Doctors Diagnose Plantar Fasciitis
Clinical Examination
Plantar fasciitis heel pain morning fix achieves accurate diagnosis primarily through clinical examination. The diagnosis is clinical — meaning history and physical findings alone confirm it in the vast majority of cases without imaging.
Doctors press firmly on the medial calcaneal tubercle — the inner heel bone attachment point of the plantar fascia — to reproduce the characteristic point tenderness. This spot tenderness is highly specific for plantar fasciitis. Furthermore, passive dorsiflexion of the toes — bending the toes upward while pressing on the heel — stretches the plantar fascia and reproduces pain in confirmed cases. Doctors also assess ankle range of movement, specifically measuring dorsiflexion restriction caused by tight calf muscles.
Imaging Studies
Imaging is not routinely required for straightforward plantar fasciitis. However, doctors order imaging when the diagnosis is uncertain, when symptoms fail to respond to treatment as expected, or when a stress fracture needs to be excluded.
Plain X-ray of the heel frequently shows a heel spur — a bony projection from the calcaneus at the plantar fascia attachment site. Furthermore, heel spurs are often blamed for plantar fasciitis pain. However, research shows that heel spurs are present in roughly 10% of the general population without symptoms. Consequently, the spur itself does not cause the pain — the degenerative fascia tissue at its base does.
Ultrasound directly visualises the plantar fascia and confirms the diagnosis by demonstrating thickening — greater than four millimetres — and loss of the normal fibrillar structure at the calcaneal attachment. Furthermore, ultrasound guides injection therapy with precision. MRI provides the most detailed tissue assessment and definitively excludes stress fracture, tumour, and other conditions when the diagnosis remains uncertain after ultrasound.
Treatment of Plantar Fasciitis
Stretching — The Most Important Treatment
Stretching is the single most evidence-supported treatment for plantar fasciitis. It directly addresses the mechanical cause — tight calf muscles and a shortened plantar fascia — that drives the condition. Furthermore, stretching reduces the tensile stress on the fascia attachment during every step.
Two specific stretches produce the strongest evidence base. The plantar fascia-specific stretch involves sitting, crossing the affected foot over the opposite knee, and pulling the toes back toward the shin until a stretch is felt along the arch. Holding for 10 seconds and repeating ten times before taking the first morning step significantly reduces morning pain in clinical trials.
The calf stretch — standing facing a wall, placing the affected foot behind, keeping the heel flat, and leaning forward — lengthens the gastrocnemius and soleus muscles and improves ankle dorsiflexion. Moreover, performing both stretches three times daily produces significantly better outcomes than stretching once daily. Consequently, patient compliance with a regular stretching programme is the single most important determinant of recovery speed.
Footwear and Orthotics
Addressing footwear is an essential component of plantar fasciitis treatment. Supportive footwear with a firm heel counter, adequate arch support, and a slight heel raise reduces the load on the plantar fascia during standing and walking. Furthermore, patients should avoid walking barefoot on hard floors — particularly first thing in the morning before the fascia has warmed up.
Prefabricated orthotics — ready-made insoles with arch support and heel cushioning — reduce plantar fascia strain effectively and at low cost. Custom orthotics — individually moulded insoles made from a cast or scan of the foot — provide greater precision for patients with significant biomechanical abnormalities. However, research shows that prefabricated orthotics achieve equivalent clinical outcomes to custom devices for most patients with standard plantar fasciitis. Consequently, custom orthotics are most appropriate for patients with complex foot structure or those who fail to improve with prefabricated options.
Physical Therapy and Load Management
Physiotherapy addresses the biomechanical drivers of plantar fasciitis beyond stretching alone. A physiotherapist assesses gait, foot posture, calf muscle strength, and ankle mobility to identify all contributing factors. Treatment includes targeted strengthening of the intrinsic foot muscles — the small muscles within the foot itself — which support the arch and reduce the load transferred to the plantar fascia during walking and running.
Eccentric calf raises — lowering the heel slowly below the step level from a raised position — strengthen the Achilles tendon and calf complex while simultaneously stretching them. This exercise reduces the tensile pull on the plantar fascia during activity. Moreover, load management — temporarily reducing high-impact activities while maintaining cardiovascular fitness through low-impact alternatives such as cycling and swimming — allows the fascia to recover without complete rest.
Taping — applying rigid sports tape or kinesiology tape to the foot to support the arch and offload the heel — provides immediate symptomatic relief during activity. Consequently, taping is a useful adjunct during the early symptomatic phase while stretching and strengthening exercises take effect.
Injections and Advanced Therapies
When stretching, footwear modification, and physiotherapy fail to provide sufficient relief after six to eight weeks, clinicians consider additional treatments. Corticosteroid injection — injecting anti-inflammatory steroid medication into the plantar fascia attachment — reduces pain significantly in the short term. Furthermore, ultrasound guidance improves injection accuracy and reduces the risk of fat pad atrophy from misdirected injection.
However, repeated corticosteroid injections carry risks including plantar fascia rupture and fat pad thinning. Consequently, most guidelines recommend limiting injections to two or three per foot and spacing them at least three months apart.
Extracorporeal shock wave therapy — called ESWT — delivers focused sound wave energy to the plantar fascia attachment. This stimulates a healing response within the degenerative tissue. Furthermore, ESWT produces significant and durable pain relief in patients with chronic plantar fasciitis — defined as symptoms lasting more than three to six months — who have failed conservative treatment. Consequently, ESWT is now the preferred intervention for chronic recalcitrant plantar fasciitis before surgery is considered.
Platelet-rich plasma injection — concentrating growth factors from the patient’s own blood and injecting them into the damaged fascia — shows promising results in clinical trials. Moreover, it may produce more durable relief than corticosteroid injection because it promotes tissue repair rather than simply reducing inflammation. However, evidence remains mixed and access varies considerably between healthcare systems.
Night Splints and Surgery
Night splints hold the foot in a neutral or slightly dorsiflexed position during sleep. This prevents the plantar fascia from shortening overnight and reduces morning pain significantly by maintaining the fascia in a lengthened position through the repair cycle. Furthermore, night splints are particularly effective for patients whose dominant symptom is severe morning pain. However, compliance can be difficult because the splint disrupts sleep comfort. Consequently, doctors typically introduce night splints for patients who have not responded adequately to stretching and footwear modification alone.
Surgery for plantar fasciitis is rare and reserved for cases that genuinely fail all conservative and minimally invasive treatments after twelve months of sustained effort. The standard procedure is plantar fascia release — partially cutting the plantar fascia at its calcaneal attachment to relieve the tension driving pain. It produces good results in carefully selected patients. However, it carries risks including arch collapse, nerve damage, and prolonged recovery. Consequently, surgery represents a last resort rather than an early intervention. For context on how surgical decisions balance risk and benefit in musculoskeletal conditions, see our article on spondylolisthesis — slipped vertebra, back pain, and treatment.
Prevention of Plantar Fasciitis
Stretching and Footwear Habits
Preventing plantar fasciitis recurrence requires addressing the same biomechanical factors that caused the initial episode. Daily calf and plantar fascia stretching — particularly before the first morning steps and after prolonged sitting — maintains the fascia in a lengthened, resilient state. Furthermore, replacing worn footwear regularly and choosing shoes with adequate arch support and cushioning reduces cumulative fascia loading.
People who stand for prolonged periods at work benefit from anti-fatigue mats, regular short walking breaks, and supportive occupational footwear. Moreover, gradual progression of physical activity — increasing training load by no more than 10% per week — prevents the overload spikes that trigger plantar fasciitis in runners and other athletes. Consequently, load management discipline is as important as stretching for long-term prevention.
Weight and Overall Foot Health
Maintaining a healthy body weight significantly reduces the mechanical load on the plantar fascia during every step of every day. Even modest weight loss produces meaningful reductions in plantar fascia stress. Furthermore, addressing contributory conditions — such as tight hip flexors, weak gluteal muscles, and poor running mechanics — reduces compensatory pronation and plantar fascia overload.
Regular foot strengthening exercises — toe curls, short foot exercises, and single-leg balance activities — build the intrinsic foot muscle strength that supports the arch independently. Consequently, a strong and flexible foot requires less passive support from the plantar fascia and adapts better to the demands of daily life and physical activity. For context on managing overlapping chronic pain conditions that can complicate foot rehabilitation, see our articles on fibromyalgia — the pain condition that is real, widely misunderstood, and treatable — and Dupuytren’s contracture — the Viking disease explained.
When to Seek Medical Help
See a doctor if heel pain persists for more than four to six weeks despite regular stretching and footwear changes. Furthermore, seek prompt assessment if the pain is severe enough to significantly limit walking, if it follows a sudden injury, if swelling or bruising accompanies the pain, or if symptoms do not follow the classic post-static dyskinesia pattern.
Consequently, early specialist assessment ensures accurate diagnosis, excludes alternative causes of heel pain, and gives access to the full range of effective treatments before the condition becomes chronic and more difficult to resolve.
Frequently Asked Questions
1. How long does plantar fasciitis take to heal?
Most cases of plantar fasciitis resolve within three to twelve months with consistent treatment. Roughly 90% of patients achieve full recovery through conservative measures without needing injections or surgery. However, recovery is significantly faster when treatment begins early and patients comply consistently with stretching and footwear modification. Consequently, starting treatment promptly after symptoms appear and committing to daily stretching gives the plantar fascia the best environment for timely healing.
2. Does plantar fasciitis go away on its own?
Some mild cases improve spontaneously over time. However, without addressing the underlying biomechanical causes — tight calves, unsupportive footwear, and excessive load — plantar fasciitis frequently becomes chronic. Furthermore, the degenerative changes that develop in the fascia over months of untreated pain make the condition progressively harder to resolve. Consequently, early treatment is significantly more effective than waiting for the problem to resolve without intervention.
3. Is it safe to exercise with plantar fasciitis?
Yes, with appropriate modification. High-impact activities that load the heel directly — running, jumping, and prolonged standing — should be temporarily reduced during acute flares. However, low-impact exercise — cycling, swimming, and aqua jogging — maintains fitness without aggravating the plantar fascia. Furthermore, targeted strengthening and stretching exercises form an active part of treatment rather than rest. Consequently, complete inactivity is neither necessary nor beneficial for most people with plantar fasciitis.
4. What is the difference between plantar fasciitis and a heel spur?
A heel spur is a bony outgrowth from the calcaneus at the plantar fascia attachment site. It develops as a response to the chronic traction stress on the fascia over time. However, the spur itself is not the primary cause of pain. Furthermore, many people have heel spurs without any pain at all. The pain in plantar fasciitis comes from the degenerative and inflammatory changes within the fascia tissue — not from the spur. Consequently, treatment targets the fascia rather than the spur.
5. Can plantar fasciitis affect both feet at the same time?
Yes. Bilateral plantar fasciitis — affecting both feet simultaneously — occurs in roughly 30% of cases. It is more common in people with systemic risk factors such as obesity, flat feet affecting both feet equally, or occupations requiring prolonged bilateral standing. Furthermore, treating one foot while ignoring biomechanical contributors allows the condition to develop in the other foot even while the first is recovering. Consequently, comprehensive assessment and treatment of both feet — including bilateral stretching and footwear correction — is recommended when bilateral symptoms are present.
References
- Height is another key factor. Strips don’t have a “regular” heel—they are truly high, usually starting from 15 cm, often 17–18 cm,
- Chenab Bridge, the world’s highest railway bridge, part of the Udhampur-Srinagar-Baramulla rail link project (USBRL)
- Martin attended the Bedford School and later studied chemistry at the University of Cambridge.
Disclaimer
This article adapts publicly available information from WHO’s Musculoskeletal Conditions page. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform and not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.