
Central Sleep Apnea: When the Problem Is in the Brain, Not the Airway
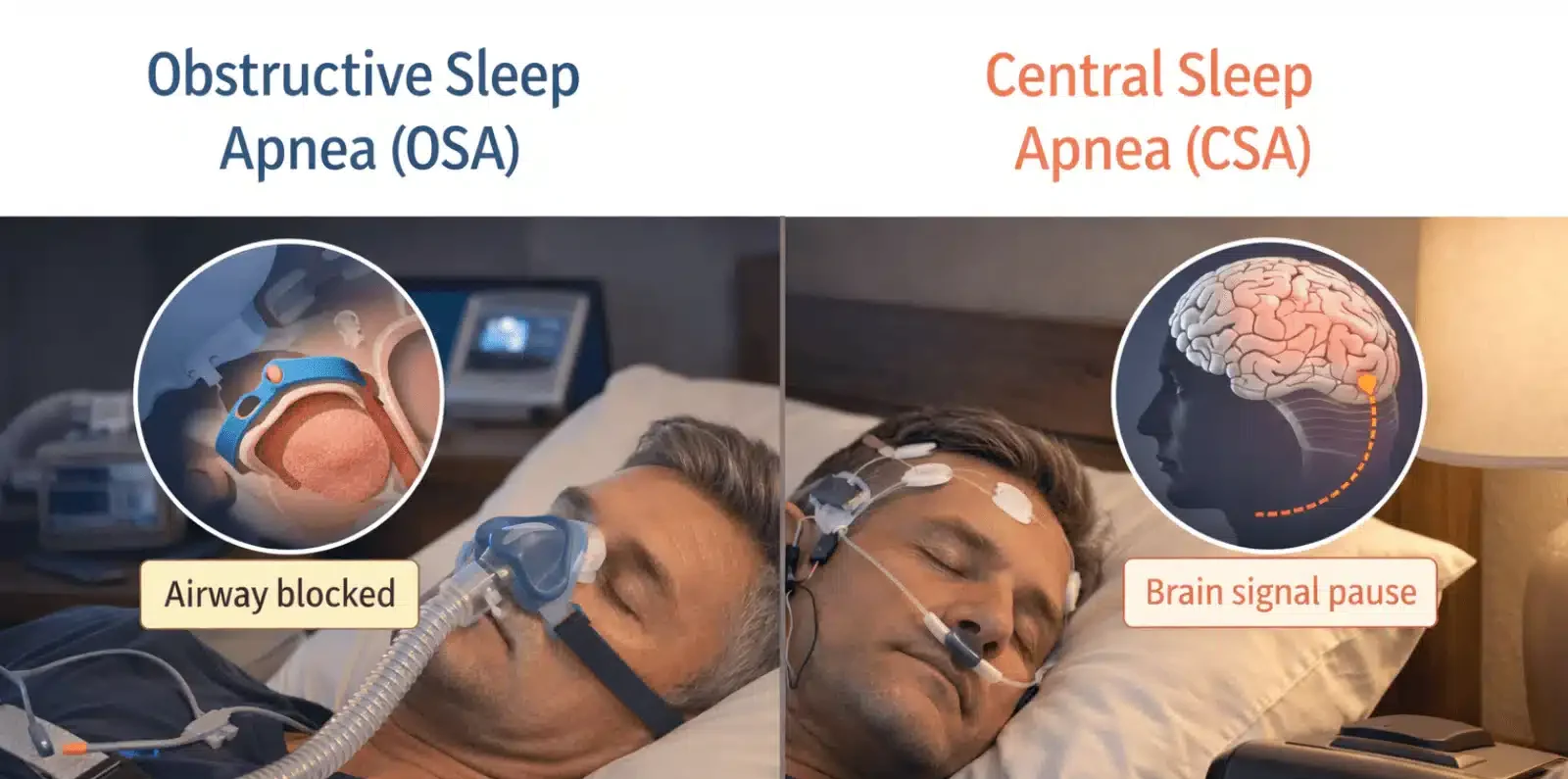
Central Sleep Apnea is a sleep disorder where breathing repeatedly stops during sleep, not because the airway is blocked, but because the brain fails to send the correct signals to the breathing muscles. Unlike Obstructive Sleep Apnea, where physical throat collapse causes breathing pauses, Central Sleep Apnea originates entirely within the nervous system. The airway remains open, yet breathing simply ceases because the brain momentarily stops commanding it.
This fundamental difference makes Central Sleep Apnea a uniquely challenging condition. It often associates with serious underlying diseases including heart failure, stroke, and opioid use, rather than occurring in isolation. Many people with Central Sleep Apnea do not snore prominently, leading to prolonged diagnostic delays while the underlying cause continues to cause harm. Understanding this condition clearly could save lives by prompting earlier recognition and more targeted treatment.
What Is Central Sleep Apnea?
Central Sleep Apnea, abbreviated as CSA, belongs to the broader category of sleep-disordered breathing. During normal sleep, the brainstem continuously monitors blood oxygen and carbon dioxide levels and adjusts breathing rate and depth accordingly. In CSA, this regulatory system malfunctions, sending no signal or an inadequate signal to the respiratory muscles during sleep.
Without a signal from the brain, the diaphragm and chest wall muscles make no effort to breathe. The result is a complete cessation of both airflow and respiratory effort, which distinguishes CSA from Obstructive Sleep Apnea, where respiratory effort continues despite the blocked airway.
The Brainstem’s Role in Breathing
The brainstem, particularly a region called the medulla oblongata, acts as the body’s automatic breathing controller. It processes chemical signals from sensors that detect rising carbon dioxide and falling oxygen in the blood. When carbon dioxide rises, the brainstem triggers a breath. In CSA, this feedback loop becomes unstable, hypersensitive, or completely absent depending on the underlying cause.
This neurological origin means that treating CSA requires addressing the brain’s signalling dysfunction, not the airway anatomy. Standard Obstructive Sleep Apnea treatments alone often prove insufficient or even counterproductive in pure CSA.
How CSA Differs From Obstructive Sleep Apnea
Understanding the distinction between Central and Obstructive Sleep Apnea matters enormously for treatment. Both conditions cause breathing pauses during sleep and produce similar consequences including fragmented sleep, daytime fatigue, and cardiovascular stress. However, their mechanisms, associated conditions, and treatments differ substantially.
Effort Versus No Effort
The defining difference lies in respiratory effort during an apnoeic episode. In Obstructive Sleep Apnea, the person tries to breathe but cannot, because the collapsed airway physically prevents airflow. Chest and abdominal muscles move visibly in their effort to overcome the obstruction. In Central Sleep Apnea, no such effort occurs. The breathing muscles remain completely still because the brain sends no command to move them.
Sleep studies measuring respiratory effort can clearly distinguish these two patterns, guiding accurate diagnosis and appropriate treatment selection.
Snoring Patterns
Loud habitual snoring is the hallmark of OSA and reflects the vibration of partially obstructed airway tissues. CSA, by contrast, typically produces little or no snoring because the airway itself is unobstructed. This absence of prominent snoring often delays clinical suspicion for CSA, particularly when the primary presentation involves fatigue or cardiovascular symptoms rather than obvious sleep disturbance.
Mixed Sleep Apnea
Some people develop complex or mixed sleep apnea, meaning a combination of both central and obstructive events. Additionally, some patients who begin CPAP therapy for Obstructive Sleep Apnea develop treatment-emergent central apneas during initial therapy. This phenomenon, called complex sleep apnea syndrome, requires modified treatment approaches.
Types of Central Sleep Apnea
CSA is not a single uniform condition. Several distinct subtypes exist, each with different underlying mechanisms and clinical contexts.
Primary Central Sleep Apnea
Primary CSA occurs without any identifiable underlying medical condition. The brainstem’s breathing control system becomes unstable for reasons that remain incompletely understood. This form is relatively rare and tends to affect older adults, particularly men. People with primary CSA often report insomnia, frequent nighttime awakenings, and excessive daytime fatigue.
Treatment focuses on stabilising the breathing control system using adaptive ventilation or other specialised therapies rather than addressing an underlying disease.
Cheyne-Stokes Breathing
Cheyne-Stokes breathing is the most clinically significant CSA subtype, strongly associating with heart failure and stroke. It produces a distinctive cyclical pattern where breathing gradually increases in depth and rate, then gradually decreases to a complete pause before the cycle restarts. This waxing and waning respiratory pattern reflects an unstable feedback loop between the brainstem and the cardiovascular system.
In heart failure, reduced cardiac output slows the delivery of blood carrying oxygen and carbon dioxide signals to the brainstem. This delay destabilises the breathing control loop, producing the characteristic Cheyne-Stokes oscillation pattern throughout the night.
High-Altitude Central Sleep Apnea
Ascending rapidly to high altitude exposes the body to lower oxygen levels. The brain responds by increasing breathing rate to compensate, a process called hypoxic ventilatory response. This hyperventilation lowers carbon dioxide below the threshold needed to stimulate breathing, causing central apnoeic pauses. High-altitude CSA typically resolves with acclimatisation over several days or descent to lower altitude.
Opioid-Induced Central Sleep Apnea
Opioid medications including morphine, oxycodone, and methadone directly suppress the brainstem’s respiratory control centres. Long-term opioid use is a leading cause of acquired CSA. The degree of respiratory suppression correlates with opioid dose and duration of use. Opioid-induced CSA carries significant mortality risk and represents an increasingly important clinical challenge given the global prevalence of opioid prescribing for chronic pain.
Treatment-Emergent Central Sleep Apnea
Some people develop central apnoeic events after starting CPAP therapy for presumed Obstructive Sleep Apnea. This treatment-emergent form, sometimes called complex sleep apnea, occurs because eliminating obstructive events unmasks an underlying instability in the brainstem’s breathing control. In many cases, this form resolves spontaneously with continued CPAP use over weeks to months.
Causes and Risk Factors for Central Sleep Apnea
CSA rarely occurs without an identifiable context. Most cases associate with specific medical conditions, medications, or physiological circumstances.
Heart Failure
Heart failure is the most common medical condition associated with CSA, particularly the Cheyne-Stokes breathing subtype. Studies suggest that up to 40 percent of people with systolic heart failure, where the heart pumps weakly, develop significant CSA during sleep. The haemodynamic instability and prolonged circulation time characteristic of heart failure directly destabilise the brainstem’s carbon dioxide sensing mechanism.
Treating heart failure effectively, with optimised medical therapy and cardiac resynchronisation therapy where appropriate, often improves associated CSA substantially.
Stroke and Neurological Conditions
Stroke affecting the brainstem or regions influencing respiratory control frequently causes CSA. The brainstem itself contains the primary respiratory rhythm generators, making it particularly vulnerable. Other neurological conditions including Parkinson’s disease, multiple system atrophy, and cervical spinal cord injury also impair the central respiratory drive and produce CSA.
In stroke survivors, CSA associates with worse neurological recovery, greater disability, and higher recurrence risk. Identifying and treating CSA in stroke rehabilitation programmes may therefore improve long-term outcomes.
Kidney Disease and Metabolic Disorders
Chronic kidney disease causes metabolic acidosis, meaning the blood becomes abnormally acidic, which stimulates increased breathing and can destabilise the carbon dioxide feedback loop. End-stage renal disease shows particularly high CSA prevalence. Metabolic alkalosis, an abnormally alkaline blood state sometimes caused by diuretic medications, conversely suppresses breathing drive and can also contribute to CSA.
Opioid and Sedative Medications
Beyond opioids, other central nervous system depressants including benzodiazepines, barbiturates, and certain anaesthetic agents suppress brainstem respiratory control and increase CSA risk. People using these medications long-term for chronic pain, anxiety, or other conditions require awareness of their respiratory effects during sleep.
Symptoms of Central Sleep Apnea
CSA produces a symptom profile that overlaps significantly with Obstructive Sleep Apnea but carries some distinguishing characteristics that clinicians and affected individuals should recognise.
Nighttime Symptoms
Witnessed breathing pauses during sleep represent the most recognisable nighttime sign of CSA. Partners or caregivers may observe the person stopping breathing, lying still without any chest movement, before suddenly gasping and resuming respiration. Unlike OSA, these pauses occur without the laboured respiratory efforts, snorting, or loud snoring that typically characterise obstructive events.
Frequent nighttime awakenings, insomnia, and an inability to maintain sleep continuity are common in CSA. Some people wake with a sensation of breathlessness or chest tightness that resolves quickly on full wakefulness.
Daytime Symptoms
Excessive daytime sleepiness affects many people with CSA, though it tends to be less severe than in comparable OSA cases. Morning headaches reflecting overnight carbon dioxide retention can occur, particularly in CSA associated with hypoventilation. Chronic fatigue, reduced exercise tolerance, and cognitive difficulties with concentration and memory are frequently reported.
Mood disturbances including irritability, anxiety, and depression commonly accompany CSA, reflecting both the effects of disrupted sleep and the psychological burden of managing serious underlying conditions.
Symptoms Reflecting Underlying Disease
Because CSA so frequently associates with significant underlying conditions, many people with CSA present primarily with the symptoms of those conditions rather than sleep-specific complaints. Breathlessness on exertion, ankle swelling, and palpitations in heart failure patients may prompt investigation that incidentally reveals CSA.
Recognising CSA as a likely complication of specific underlying conditions drives more systematic and proactive sleep assessment in high-risk patient groups.
Diagnosing Central Sleep Apnea
Accurate CSA diagnosis requires objective sleep testing combined with targeted investigation of underlying causes. Clinical suspicion alone cannot reliably identify or characterise CSA.
Polysomnography
In-laboratory polysomnography remains the gold standard diagnostic test for CSA. This comprehensive overnight sleep study records brain activity, eye movements, muscle activity, heart rhythm, airflow, respiratory effort, oxygen saturation, and body position simultaneously. Crucially, polysomnography measures respiratory effort using thoracic and abdominal bands, allowing direct differentiation between central apnoeic events, where no effort occurs, and obstructive events, where effort continues.
The Apnoea-Hypopnoea Index (AHI) quantifies sleep-disordered breathing severity. A predominantly central AHI, with central events comprising more than half of all recorded events, establishes the diagnosis of CSA.
Home Sleep Testing Limitations
Standard home sleep testing devices measure airflow and oxygen saturation but cannot reliably measure respiratory effort with the precision needed to distinguish central from obstructive events. Consequently, home sleep testing is generally inadequate for CSA diagnosis. People with suspected CSA require full in-laboratory polysomnography for accurate diagnosis and characterisation.
Investigating Underlying Causes
Every person diagnosed with CSA requires thorough investigation for underlying medical conditions. Cardiac assessment including echocardiography identifies heart failure and evaluates cardiac function. Brain imaging detects stroke or structural neurological abnormalities. Blood tests assess kidney function, thyroid function, and metabolic parameters. A comprehensive medication review identifies opioids or other respiratory depressants contributing to CSA.
Identifying and addressing underlying conditions fundamentally shapes treatment strategy and long-term prognosis in CSA.
Treatment of Central Sleep Apnea
Treating CSA requires a dual approach: addressing the underlying cause where possible and using specialised ventilatory support to stabilise breathing during sleep.
Treating the Underlying Condition
In many CSA cases, optimising treatment of the underlying condition produces significant improvement in sleep-disordered breathing. Optimising heart failure therapy with medications, cardiac devices, and lifestyle modifications reduces Cheyne-Stokes breathing severity in many patients. Reducing or eliminating opioid doses, where clinically feasible, improves opioid-induced CSA substantially.
Neurological rehabilitation after stroke and management of other contributing conditions all contribute to CSA improvement as part of a comprehensive treatment approach.
Adaptive Servo-Ventilation
Adaptive Servo-Ventilation (ASV) is a sophisticated form of non-invasive ventilation specifically designed for CSA treatment. ASV continuously monitors the patient’s breathing pattern and automatically adjusts pressure support to counteract the cyclical ventilatory instability characteristic of CSA. When breathing slows or stops, ASV increases support to stimulate a breath. When breathing is adequate, it reduces support to avoid over-ventilation.
ASV shows superiority over standard CPAP and bilevel positive airway pressure (BiPAP) for most CSA subtypes. However, an important exception exists for CSA associated with heart failure and reduced ejection fraction, where a major clinical trial demonstrated increased mortality with ASV use. This finding has significantly changed clinical guidelines, restricting ASV use in this specific patient group.
CPAP and BiPAP Therapy
Standard CPAP therapy plays a limited role in pure CSA but effectively treats treatment-emergent and mixed CSA forms. For many patients whose central apnoeic events emerge after starting CPAP for OSA, continued CPAP use over weeks resolves the central events as the brainstem adapts to the new pressure environment.
BiPAP therapy, delivering separate higher inspiratory and lower expiratory pressures, provides ventilatory assistance during both phases of breathing. It suits CSA cases associated with hypoventilation, such as those caused by neuromuscular disease or chronic respiratory failure, where additional breathing support beyond simple airway pressure proves necessary.
Supplemental Oxygen
Supplemental oxygen therapy reduces hypoxic drive instability in selected CSA patients, particularly those with high-altitude CSA and some heart failure patients. By maintaining adequate oxygen levels, supplemental oxygen reduces the hypoxic stimulus that perpetuates ventilatory oscillation in susceptible individuals.
Oxygen therapy alone rarely suffices for severe CSA but provides a useful adjunct to ventilatory support strategies in carefully selected cases.
Pharmacological Approaches
Acetazolamide, a carbonic anhydrase inhibitor medication, promotes mild metabolic acidosis that stimulates breathing drive. It shows effectiveness for high-altitude CSA and some cases of primary CSA. The medication improves carbon dioxide sensitivity and stabilises the brainstem’s breathing control loop in susceptible individuals.
Theophylline, a respiratory stimulant, has historical use in CSA but carries significant cardiovascular side effects limiting its clinical utility. Pharmacological approaches remain adjunctive rather than primary treatments in most CSA management strategies.
Central Sleep Apnea and Heart Failure
The relationship between CSA and heart failure deserves particular attention given its clinical importance and complexity.
Bidirectional Harm
CSA and heart failure inflict harm on each other in a vicious cycle. Heart failure causes CSA through haemodynamic instability and delayed circulation. CSA then worsens heart failure through repeated overnight hypoxia, sympathetic nervous system activation, and increased cardiac workload. Breaking this cycle through effective treatment of both conditions simultaneously is the central challenge of managing CSA in heart failure.
Treatment Caution
The SERVE-HF trial, a landmark randomised controlled trial published in 2015, demonstrated that ASV therapy increased all-cause mortality and cardiovascular mortality in heart failure patients with reduced ejection fraction and predominantly central apnoeic events. This unexpected finding fundamentally changed clinical practice. Clinicians now exercise great caution before initiating ASV in heart failure patients, restricting its use to cases where heart function is preserved or reduced ejection fraction has been excluded.
This caution underscores the importance of precise CSA subtype characterisation and comprehensive cardiac assessment before treatment selection.
Living With Central Sleep Apnea
Managing CSA long-term requires sustained engagement with specialist care, ongoing monitoring, and attention to the physical and psychological dimensions of chronic illness.
Long-Term Monitoring
Regular follow-up with a sleep medicine specialist ensures that treatment remains effective as the underlying condition and disease activity evolve. Repeat sleep studies assess treatment response and detect changes in apnoea pattern over time. Cardiac monitoring remains essential in heart failure patients with CSA.
Consistent device usage and prompt reporting of new or worsening symptoms enable timely treatment adjustments before significant deterioration occurs.
Psychological and Social Support
Living with CSA and its associated conditions carries a substantial psychological burden. Anxiety about overnight breathing, depression, and social isolation due to fatigue and disability all require attention. Access to psychological support, peer networks, and patient organisations significantly improves overall wellbeing and treatment adherence in people managing this complex condition long-term.
Frequently Asked Questions
What is Central Sleep Apnea?
Central Sleep Apnea is a sleep disorder where breathing repeatedly stops during sleep because the brain fails to send adequate signals to the breathing muscles. Unlike Obstructive Sleep Apnea, where a blocked airway causes breathing pauses, the airway in CSA remains physically open. The problem originates in the brainstem’s respiratory control system rather than in the throat anatomy.
How is Central Sleep Apnea different from Obstructive Sleep Apnea?
The fundamental difference lies in respiratory effort. In Obstructive Sleep Apnea, the person tries to breathe but a collapsed airway prevents airflow. In Central Sleep Apnea, no breathing effort occurs because the brain sends no signal to the breathing muscles. CSA typically produces less snoring, associates with different underlying conditions, and requires different treatment strategies compared to OSA.
What causes Central Sleep Apnea?
CSA most commonly associates with underlying medical conditions including heart failure, stroke, kidney disease, and neurological disorders. Opioid and other central nervous system depressant medications suppress brainstem respiratory control and cause CSA. High altitude triggers a specific form. Primary CSA occurs without identifiable cause, though this form is relatively uncommon.
Can Central Sleep Apnea be treated?
Yes, though treatment is more complex than for Obstructive Sleep Apnea. Addressing the underlying condition forms the foundation of management. Adaptive Servo-Ventilation effectively stabilises breathing in many CSA subtypes, though it carries important restrictions in heart failure patients. CPAP, BiPAP, supplemental oxygen, and medications such as acetazolamide all have roles in specific CSA presentations.
Is Central Sleep Apnea dangerous?
Yes, particularly when associated with serious underlying conditions such as heart failure or stroke. CSA causes recurrent overnight hypoxia, sleep fragmentation, and cardiovascular stress. It associates with increased mortality in heart failure patients. Prompt diagnosis and appropriate treatment are essential to reduce the health risks CSA imposes, both independently and through its interaction with underlying diseases.
How is Central Sleep Apnea diagnosed?
Central Sleep Apnea requires in-laboratory polysomnography for accurate diagnosis. This overnight sleep study records respiratory airflow and effort simultaneously, allowing central apnoeic events to be distinguished from obstructive ones. Home sleep tests generally cannot reliably diagnose CSA. Comprehensive investigation for underlying medical causes, including cardiac assessment and neurological evaluation, follows confirmed CSA diagnosis.
Disclaimer:
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis, treatment, or medical guidance related to any health condition.
References:
- Obstructive Sleep Apnea is far more than a nighttime nuisance that makes people snore loudly.
- World COPD (Chronic Obstructive Pulmonary Disease) Day is an annual event observed on the third Wednesday of November each year.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.