
Bursitis: Inflamed Fluid Sacs Behind Shoulder, Hip, and Knee Pain
Most people have never heard of a bursa. However, bursae — the plural of bursa — play a quiet but essential role in keeping the body moving smoothly and without pain. These small, fluid-filled sacs sit at strategic points throughout the musculoskeletal system. They cushion the spaces between bones, tendons, and muscles — reducing friction and protecting delicate tissue from the mechanical wear of daily movement.
When a bursa becomes inflamed, it swells with excess fluid and causes the sharp, aching, or burning pain that patients and doctors call bursitis. The shoulder, hip, and knee are the most commonly affected regions — but bursitis can develop wherever a bursa exists, which includes over 150 locations throughout the body. Furthermore, bursitis is frequently mistaken for arthritis, muscle strain, or tendinopathy — causing unnecessary delays in diagnosis and treatment.
Bursitis inflamed fluid sac shoulder hip knee pain is the central focus of this article. Millions of people worldwide live with bursitis-related pain that significantly limits their work, sport, and daily activities. Consequently, understanding what inflames a bursa, which symptoms point to bursitis rather than other conditions, and which treatments genuinely resolve it gives patients a clear path to faster recovery and prevention of recurrence.
Quick Answer
Bursitis is inflammation of a bursa — a small fluid-filled sac that cushions bones, tendons, and muscles at joints. It causes localised pain, swelling, and tenderness at the affected site. The shoulder, hip, and knee are most commonly affected. Treatment combines rest, anti-inflammatory medication, physiotherapy, and — when needed — corticosteroid injection or aspiration.
What Is a Bursa and What Does It Do?
The Structure and Function of Bursae
A bursa is a thin-walled sac lined with synovial membrane — the same tissue that lines joint cavities. This lining produces a small amount of synovial fluid — a viscous, lubricating liquid — that fills the sac and allows the structures on either side of it to glide smoothly past each other during movement.
Bursae serve as biological ball bearings. They reduce friction at points where tendons or muscles pass over bony prominences — areas where repeated movement without cushioning would generate damaging shear forces on soft tissue. Furthermore, they absorb the compressive forces produced during kneeling, leaning, or repetitive impact activity. Without bursae, the tendons, muscles, and bones they separate would grind against each other — generating pain, tissue damage, and progressive functional decline.
Where Bursae Are Located
The body contains over 150 bursae. Some are present at birth — called anatomical bursae — and develop as part of normal musculoskeletal anatomy. Others — called adventitious bursae — develop in response to abnormal or excessive mechanical pressure over time. The clinically most important bursae sit at the shoulder, hip, knee, elbow, heel, and around the pelvis.
The subacromial bursa sits between the rotator cuff tendons and the acromion — the bony roof of the shoulder. The trochanteric bursa sits over the greater trochanter — the prominent bony landmark on the outer hip. The prepatellar bursa sits directly in front of the kneecap. Moreover, the retrocalcaneal bursa cushions the space between the Achilles tendon and the heel bone. Consequently, bursitis can present as shoulder, hip, knee, or heel pain depending on which bursa is affected.
What Causes Bursitis?
Repetitive Mechanical Stress
Bursitis inflamed fluid sac shoulder hip knee pain most commonly results from repetitive mechanical stress on a bursa — the cumulative effect of repeated compression or friction that exceeds the bursa’s tolerance and triggers an inflammatory response. Repetitive overhead arm movements inflame the subacromial bursa. Prolonged kneeling on hard surfaces inflames the prepatellar bursa — earning it the traditional occupational name housemaid’s knee or carpet layer’s knee.
Prolonged sitting on hard surfaces inflames the ischial bursae — located over the sitting bones of the pelvis — producing pain during prolonged sitting that office workers and cyclists frequently experience. Moreover, running with a tight iliotibial band or abnormal hip mechanics inflames the trochanteric bursa and produces the burning lateral hip pain characteristic of greater trochanteric pain syndrome. Consequently, repetitive movement and sustained pressure on specific bursae are the most common triggers in clinical practice.
Trauma and Sudden Loading
A single acute traumatic event can trigger bursitis. A direct blow to the kneecap — from a fall or sporting impact — inflames the prepatellar bursa rapidly. Impact to the elbow inflames the olecranon bursa — the prominent soft swelling that sometimes develops over the bony tip of the elbow after trauma. Furthermore, sudden unaccustomed activity — a person who rarely exercises suddenly engaging in heavy manual work or an intense training session — can overload bursae that lack the adaptive capacity built by gradual conditioning.
Systemic Conditions and Infection
Several systemic conditions significantly increase bursitis risk. Rheumatoid arthritis — an autoimmune condition that inflames synovial tissue throughout the body — frequently causes bursitis at multiple sites simultaneously. Gout — a condition in which uric acid crystals deposit in soft tissues — can trigger acute bursitis. Pseudogout, caused by calcium pyrophosphate crystal deposition, produces a similar pattern. Furthermore, diabetes, hypothyroidism, and chronic kidney disease all increase susceptibility to bursitis through mechanisms involving altered tissue metabolism and immune function. For context on how kidney disease affects musculoskeletal tissue, see our article on chronic kidney disease and bone health.
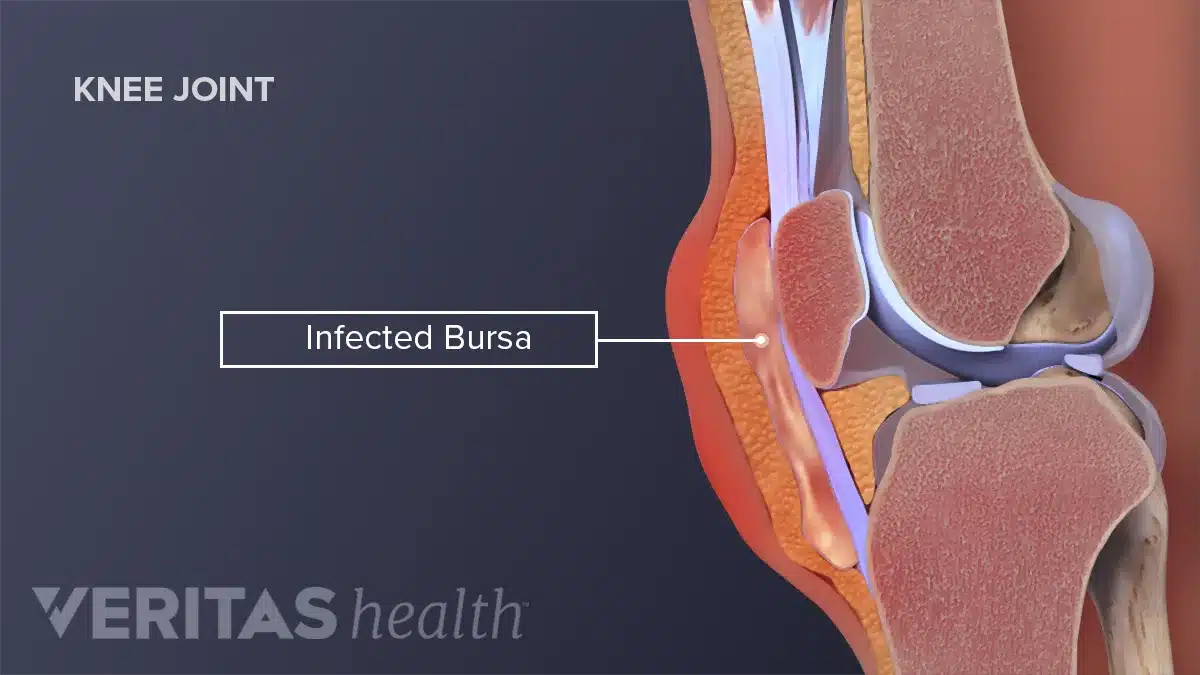
Septic bursitis — infection of a bursa — represents a clinically important and more dangerous cause of bursitis. Bacteria — most commonly Staphylococcus aureus — enter the bursa through a small skin break, abrasion, or puncture wound overlying the bursa. The olecranon and prepatellar bursae are most commonly affected because they sit just beneath the skin surface with minimal overlying tissue. Septic bursitis causes more intense redness, warmth, and swelling than non-infective bursitis — and it requires aspiration, culture, and antibiotic treatment rather than simple anti-inflammatory management. For context on how bacterial infections destroy musculoskeletal tissue, see our article on septic arthritis — the joint infection that destroys cartilage.
Symptoms of Bursitis
The Core Symptom Pattern
Bursitis inflamed fluid sac shoulder hip knee pain produces a characteristic symptom pattern. Localised pain — precisely over the affected bursa rather than diffusely throughout the joint — is the defining feature. The pain is typically described as aching, burning, or sharp. It worsens with the specific movements or positions that compress or stretch the inflamed bursa and eases with rest and avoidance of provocative activity.
Tenderness on direct palpation — pressing on the skin directly over the inflamed bursa — reproduces the pain reliably and helps localise the diagnosis clinically. Furthermore, visible or palpable swelling develops as the bursa fills with excess inflammatory fluid. The swelling is soft and fluctuant — meaning it has a fluid-filled quality that distinguishes it from the bony swelling of arthritis or the firm swelling of a solid tumour. Consequently, the combination of localised tenderness and soft swelling directly over a known bursa location provides strong clinical evidence for bursitis.
Shoulder Bursitis Symptoms
Subacromial bursitis — inflammation of the bursa beneath the acromion — is the most common cause of shoulder bursitis and produces a painful arc of shoulder movement. The pain is worst when lifting the arm between 60 and 120 degrees — the range where the subacromial space narrows and the inflamed bursa is compressed. Furthermore, reaching overhead, reaching behind the back, and lying on the affected shoulder at night all intensify the pain.
Subacromial bursitis frequently coexists with rotator cuff tendinopathy or partial rotator cuff tears — making clinical distinction between these conditions difficult without imaging. For context on how the rotator cuff and subacromial bursa interact in shoulder pain, see our article on rotator cuff tear — symptoms, diagnosis, and when surgery is actually needed.
Hip and Knee Bursitis Symptoms
Trochanteric bursitis — now more accurately called greater trochanteric pain syndrome — produces pain over the outer hip and thigh. The pain worsens when lying on the affected side, walking, climbing stairs, or crossing the legs. Many patients describe a burning or aching pain that radiates down the outer thigh. Furthermore, direct pressure over the greater trochanter — the bony prominence on the outer hip felt through the lateral thigh — reproduces the pain precisely.
Prepatellar bursitis produces a soft, visible swelling directly over the front of the kneecap. The knee itself moves through a full range of motion without significant pain — distinguishing prepatellar bursitis from conditions affecting the joint itself. However, kneeling and direct pressure on the swollen area produce sharp pain. Moreover, infrapatellar bursitis — inflammation of the bursa below the kneecap — causes pain and tenderness in the lower patellar tendon region. Consequently, the precise location of knee swelling — above, over, or below the kneecap — helps localise which bursa is affected.
How Doctors Diagnose Bursitis
Clinical Assessment
Diagnosing bursitis inflamed fluid sac shoulder hip knee pain relies primarily on clinical assessment. A careful history establishes the location, character, and duration of pain — as well as any preceding activity, trauma, or systemic condition. Physical examination identifies the precise site of maximum tenderness and any palpable swelling.
Specific clinical tests help confirm the diagnosis at each site. The Neer impingement test and Hawkins-Kennedy test reproduce subacromial pain by compressing the subacromial bursa under the acromion. The FABER test — flexion, abduction, and external rotation of the hip — reproduces trochanteric bursitis pain by stretching the iliotibial band over the greater trochanter. Direct palpation of the greater trochanter in side-lying reproduces the characteristic tenderness of trochanteric bursitis reliably. Consequently, experienced clinicians diagnose most cases of bursitis through history and examination alone without requiring imaging.
Imaging and Aspiration
Imaging provides confirmatory information when clinical findings are uncertain or when the diagnosis needs to be distinguished from other conditions. Ultrasound is the first-line imaging investigation for bursitis. It directly visualises bursal fluid — confirming inflammation — and distinguishes bursitis from adjacent tendon tears, joint effusions, and soft tissue masses. Furthermore, ultrasound guides aspiration and injection procedures with precision — improving accuracy and reducing the risk of neurovascular injury.
MRI provides the most comprehensive assessment when multiple pathologies coexist — for example, when subacromial bursitis accompanies a suspected rotator cuff tear or when trochanteric bursitis coexists with gluteal tendinopathy. Moreover, MRI excludes bone marrow pathology and stress fractures that occasionally mimic bursitis pain clinically. For context on how imaging guides musculoskeletal diagnosis, see our article on osteoarthritis — inflammation, causes, and what actually helps.
Bursal aspiration — withdrawing fluid from the inflamed bursa — is essential when septic bursitis is suspected. The fluid colour, turbidity, cell count, Gram stain, and culture determine whether the bursitis is infective or non-infective. Furthermore, crystal analysis of aspirated fluid identifies gout or pseudogout as an underlying cause. Consequently, aspiration provides both diagnostic and therapeutic benefit — removing inflammatory fluid relieves pain and allows fluid analysis to guide treatment.
Treatment of Bursitis
Rest and Activity Modification
Treatment of bursitis inflamed fluid sac shoulder hip knee pain begins with reducing the mechanical stress that triggered and perpetuates the inflammation. Identifying and modifying the aggravating activity — whether overhead work, kneeling, running technique, or sitting posture — removes the primary driver of bursal irritation. Furthermore, protective padding reduces direct pressure on superficial bursae — particularly the prepatellar and olecranon bursae — during activities that cannot be avoided entirely.
Complete rest is not necessary or advisable for most bursitis. Maintaining gentle movement within pain limits preserves tissue flexibility and prevents the stiffness and muscle weakness that worsen outcomes. Consequently, activity modification rather than complete immobilisation is the appropriate initial management for the majority of non-infective bursitis cases.
Anti-Inflammatory Medications and Ice
Non-steroidal anti-inflammatory drugs — NSAIDs including ibuprofen, naproxen, and diclofenac — reduce both pain and bursal inflammation effectively. Topical NSAIDs applied directly over the affected bursa achieve local anti-inflammatory effects with minimal systemic drug exposure. Furthermore, oral NSAIDs provide more powerful systemic relief for cases with significant pain and swelling — but carry gastrointestinal, cardiovascular, and kidney risks with prolonged use.
Ice application to the affected bursa for fifteen to twenty minutes three to four times daily reduces acute inflammation and provides analgesic benefit without drug side effects. Moreover, ice is particularly effective in the first forty-eight to seventy-two hours after a traumatic bursitis episode — limiting the initial inflammatory response before it becomes established. Consequently, ice and topical NSAIDs together provide safe and effective first-line symptom control for most acute bursitis cases.
Physiotherapy
Physiotherapy addresses the biomechanical causes of bursitis rather than simply managing its symptoms. A physiotherapist identifies the specific movement patterns, muscle weaknesses, and postural abnormalities that generate excessive mechanical stress on the affected bursa. Targeted strengthening and flexibility exercises then correct these underlying drivers.
For subacromial bursitis, rotator cuff and scapular stabiliser strengthening reduces the impingement of the bursa between the rotator cuff and acromion during shoulder movement. For trochanteric bursitis, gluteal strengthening — particularly the gluteus medius — reduces the dynamic compression of the trochanteric bursa during walking and single-leg activities. Moreover, for prepatellar bursitis, quadriceps strengthening and patellofemoral alignment correction reduce the compressive forces transmitted to the bursa during kneeling and stair climbing.
Load management — progressively reintroducing activity at a rate that allows tissue adaptation without triggering recurrence — is an essential component of physiotherapy for bursitis. Consequently, patients who address the underlying biomechanical causes with physiotherapy experience far lower recurrence rates than those who rely on injections and medications alone. For context on how tendon and bursa rehabilitation principles apply across musculoskeletal conditions, see our article on plantar fasciitis — why your heel hurts and how to fix it.
Corticosteroid Injection
Corticosteroid injection — delivering anti-inflammatory steroid medication directly into the inflamed bursa — provides rapid and significant pain relief when conservative measures prove insufficient. The injection reduces bursal inflammation dramatically within days. Furthermore, ultrasound guidance improves injection precision — ensuring the medication reaches the bursa rather than adjacent structures.
Corticosteroid injection is most effective when combined with physiotherapy rather than used as a standalone treatment. Injecting alone reduces pain but does not address the biomechanical cause — making recurrence highly likely. However, the pain relief an injection provides creates a window during which physiotherapy can begin more effectively without pain limitation. Moreover, most guidelines recommend limiting injections to three per site per year — because repeated high-dose steroid exposure weakens adjacent tendons and potentially accelerates tissue degeneration. Consequently, injection is a useful adjunct rather than a primary treatment strategy.
Aspiration and Antibiotics for Septic Bursitis
Septic bursitis requires specific management distinct from non-infective bursitis. Aspiration of the infected bursa provides immediate relief and yields fluid for Gram stain, culture, and sensitivity testing. Oral antibiotics — typically covering Staphylococcus aureus — begin immediately after aspiration while culture results are pending.
Most cases of uncomplicated septic bursitis — particularly prepatellar and olecranon bursitis — respond well to aspiration, oral antibiotics, and wound care without requiring surgical drainage. However, cases with cellulitis — spreading skin infection — systemic illness, immunocompromise, or failure to improve within forty-eight to seventy-two hours of oral antibiotics require intravenous antibiotic therapy and consideration of surgical bursal excision. Consequently, close clinical review within forty-eight hours of initiating antibiotic treatment is essential for all patients with septic bursitis. For context on how bacterial joint and bursal infections are managed, see our article on reactive arthritis — when infection triggers joint pain.
Surgery for Chronic or Recurrent Bursitis
Surgery is rarely required for bursitis. However, in cases where bursitis becomes chronic — persisting despite adequate conservative treatment and repeated injections — surgical bursal excision produces definitive resolution. The procedure — called bursectomy — removes the entire inflamed bursa. New bursae do not reliably regenerate after excision. Consequently, bursectomy prevents recurrence of the specific bursitis but requires careful patient selection to ensure surgical risk and recovery are justified by the degree of disability the chronic bursitis is causing.
Arthroscopic bursectomy — keyhole removal of the bursa — has largely replaced open surgery for subacromial and trochanteric bursitis in most centres. It achieves complete bursal excision through small incisions, reduces recovery time, and allows simultaneous treatment of associated pathology — including rotator cuff repair and acromioplasty at the shoulder. Furthermore, open bursectomy remains the preferred approach for the olecranon and prepatellar bursae where the superficial anatomy makes open surgery straightforward and arthroscopic access less practical.
Prevention of Bursitis
Addressing Mechanical Triggers
Preventing bursitis recurrence requires eliminating or modifying the mechanical triggers that caused the initial episode. Using padded kneeling supports for occupational or recreational kneeling protects the prepatellar bursa. Ergonomic workplace assessment reduces sustained compression of shoulder and hip bursae during work tasks. Furthermore, avoiding prolonged sitting on hard surfaces without adequate cushioning reduces ischial and trochanteric bursal stress.
Footwear assessment is particularly important for trochanteric and retrocalcaneal bursitis — because abnormal foot pronation and inappropriate footwear alter hip and Achilles mechanics in ways that increase bursal loading. Consequently, addressing footwear and orthotics as part of a holistic prevention strategy reduces both the primary risk and recurrence risk for several common bursitis types.
Exercise and Conditioning
Maintaining the muscle strength and flexibility that support bursae against mechanical stress is the most sustainable long-term preventive strategy. Strong gluteal muscles protect the trochanteric bursa. Strong rotator cuff and scapular stabiliser muscles protect the subacromial bursa. Moreover, flexible calf muscles and a mobile ankle joint protect the retrocalcaneal bursa.
Gradual progression of exercise load — increasing training volume, intensity, and frequency by no more than 10% per week — prevents the sudden load spikes that trigger bursitis in athletes and active individuals. Furthermore, adequate warm-up before activity and cool-down stretching afterward maintain the tissue extensibility that allows bursae to function within their normal range without excessive stress. Consequently, a consistent conditioning programme significantly reduces lifetime bursitis risk for physically active people.
When to Seek Medical Help
See a doctor promptly if bursal swelling increases rapidly, if the overlying skin becomes red and warm in a spreading pattern, or if fever develops alongside bursal pain and swelling. These features suggest septic bursitis requiring urgent aspiration and antibiotic treatment.
Furthermore, seek medical assessment if bursitis pain limits daily activities for more than two to three weeks without improvement, if pain wakes you from sleep consistently, or if swelling is large and tense rather than soft and fluctuant. Consequently, early assessment and accurate diagnosis ensure the correct treatment pathway and prevent the progression from acute to chronic bursitis.
Frequently Asked Questions
1. How long does bursitis take to heal?
Acute bursitis triggered by a specific event — such as a fall or sudden heavy activity — typically resolves within two to six weeks with appropriate rest, anti-inflammatory treatment, and physiotherapy. Chronic bursitis — developing gradually from repetitive stress — takes longer to resolve and requires more sustained treatment including addressing biomechanical causes. Furthermore, recurrence is common when the underlying mechanical trigger is not corrected. Consequently, recovery speed depends far more on addressing the cause than on treating the symptoms alone.
2. Is bursitis the same as arthritis?
No. Bursitis and arthritis are different conditions that can both cause joint pain. Bursitis involves inflammation of the fluid-filled sac cushioning the outside of a joint — not the joint itself. Arthritis involves damage or inflammation within the joint — affecting cartilage, synovium, and bone. Furthermore, bursitis pain is typically localised to the specific bursa location rather than diffusely throughout the joint, and joint movement is often preserved in bursitis while it is restricted and painful in arthritis. Consequently, accurate diagnosis distinguishes the two conditions and guides appropriate treatment.
3. Can bursitis go away on its own?
Mild acute bursitis sometimes resolves spontaneously with simple rest and activity modification within a few weeks. However, bursitis that persists beyond three to four weeks without treatment frequently becomes chronic — with bursal wall thickening and recurrent fluid accumulation that makes resolution increasingly difficult. Furthermore, chronic bursitis carries a high recurrence risk even after successful treatment if the underlying mechanical cause remains unaddressed. Consequently, early treatment and cause identification significantly improve the probability of complete resolution.
4. What is the difference between septic bursitis and non-septic bursitis?
Non-septic bursitis results from mechanical stress, trauma, or systemic inflammatory conditions — without bacterial infection. It responds to anti-inflammatory medications, physiotherapy, and corticosteroid injection. Septic bursitis results from bacterial infection of the bursa — most commonly Staphylococcus aureus entering through a skin breach. It requires aspiration for culture, antibiotic treatment, and close monitoring. Furthermore, giving corticosteroid injections to a septic bursa — mistaking it for non-infective bursitis — worsens the infection significantly. Consequently, distinguishing the two forms through aspiration and fluid analysis is essential before any injection is given.
5. Can bursitis affect children?
Yes, though it is less common in children than in adults. Septic bursitis — particularly olecranon and prepatellar bursitis — occurs in active children following minor skin injuries over these bursae. Furthermore, in adolescent athletes, subacromial and trochanteric bursitis can develop from sports training overload. Consequently, any child with localised soft swelling over a bony prominence — particularly with overlying skin changes — requires medical assessment to distinguish septic from non-septic bursitis and to initiate appropriate treatment promptly.
References
- You can feel hip pain at any stage of life, including childhood, young adulthood and the middle years.
- Rheumatoid arthritis is a chronic autoimmune disease that affects millions globally. It causes persistent inflammation, severe pain
- Scientists have made a groundbreaking discovery of a planet that appears to be influencing its host star in a dramatic way.
Disclaimer
This article adapts publicly available information from WHO’s Musculoskeletal Conditions page. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform and not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.