
Pneumothorax: When Air Gets Into the Space Around the Lung
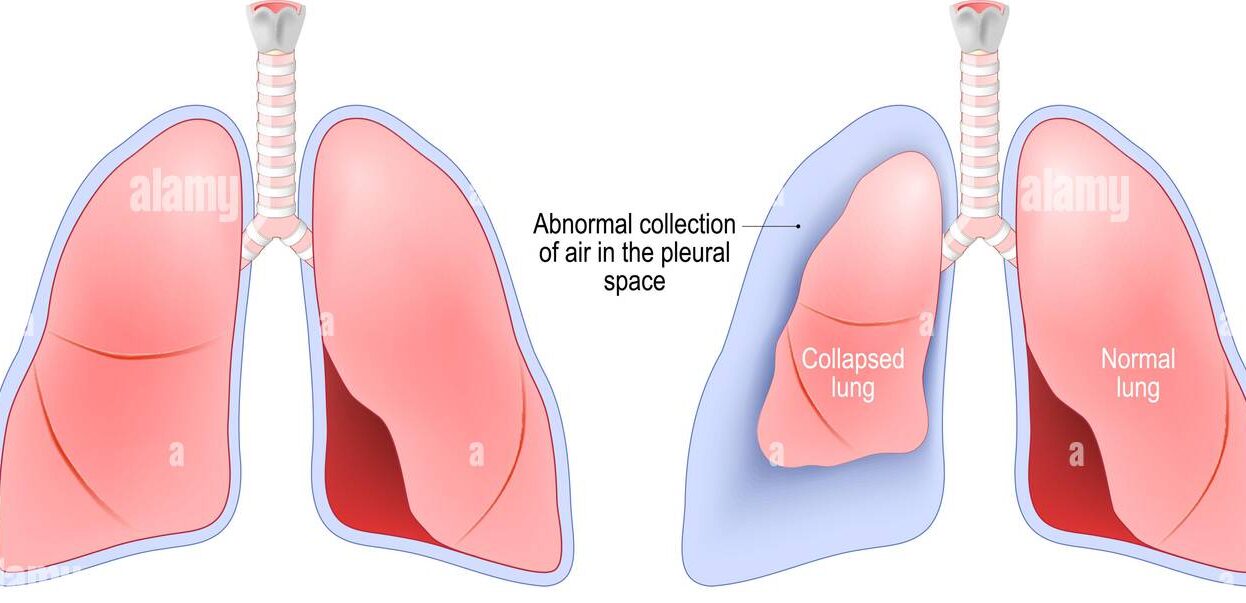
Pneumothorax is a serious and potentially life-threatening condition that occurs when air leaks into the space between the lung and the chest wall. This space, called the pleural cavity, normally contains only a thin film of fluid that helps the lung slide smoothly during breathing. When air enters this space, it disrupts the delicate pressure balance that keeps the lung inflated, causing it to partially or completely collapse.
The word pneumothorax combines the Greek words for air and chest. Most people encounter this condition as a sudden, frightening event involving sharp chest pain and unexpected breathlessness. For some, it strikes without warning during routine activity or even at rest. For others, it follows chest trauma or an underlying lung disease. Understanding pneumothorax fully, from its causes to its treatment and prevention, empowers people to seek timely care and achieve the best possible outcome.
What Is Pneumothorax?
The lungs sit inside the chest cavity and are surrounded by two thin membranes called the pleura. The inner membrane, called the visceral pleura, covers the lung surface directly. The outer membrane, called the parietal pleura, lines the inside of the chest wall. Between these two layers lies the pleural space, a narrow gap maintained at slightly negative pressure.
This negative pressure is essential. It acts like suction, keeping the lung expanded against the chest wall and enabling it to inflate with each breath. When air enters the pleural space through a hole in either layer, this negative pressure is lost. The lung recoils inward, collapsing partially or fully depending on how much air accumulates.
Why Pressure Matters So Much
The mechanics of breathing depend entirely on pressure differences. When the diaphragm contracts and the chest wall expands, pressure inside the chest drops below atmospheric pressure. Air flows into the lungs along this pressure gradient. When pneumothorax introduces atmospheric air into the pleural space, this gradient collapses on the affected side, impairing or eliminating effective ventilation of that lung.
Understanding this pressure mechanism explains why pneumothorax causes breathlessness even when the opposite lung continues functioning normally. The affected lung simply cannot expand as it should, reducing the total oxygen the body receives with each breath.
Types of Pneumothorax
Doctors classify pneumothorax into several types based on the underlying cause and the mechanism of air entry. Each type has distinct clinical implications.
Primary Spontaneous Pneumothorax
Primary spontaneous pneumothorax occurs in people with no known underlying lung disease. It most commonly affects tall, lean young men between 15 and 35 years old. The typical cause is the rupture of a small air-filled blister on the lung surface called a bleb or bulla. These blebs form near the apex, meaning the top, of the lung, often without any identifiable triggering event.
Despite occurring in otherwise healthy people, primary spontaneous pneumothorax can cause significant symptoms and carries a recurrence risk of up to 50 percent after a first episode without definitive treatment.
Secondary Spontaneous Pneumothorax
Secondary spontaneous pneumothorax develops as a complication of existing lung disease. Conditions including chronic obstructive pulmonary disease (COPD), asthma, cystic fibrosis, pulmonary fibrosis, tuberculosis, and pneumocystis pneumonia all increase pneumothorax risk. Because these individuals already have compromised lung function, even a small pneumothorax can cause severe respiratory distress.
Secondary spontaneous pneumothorax carries substantially higher morbidity and mortality than the primary form and requires more aggressive management.
Traumatic Pneumothorax
Traumatic pneumothorax results from direct chest injury. Penetrating chest wounds from stab injuries or gunshots create an obvious pathway for air entry. Blunt trauma from road accidents, falls, or sports injuries can fracture ribs that puncture the pleura. Medical procedures including central venous catheter insertion, lung biopsy, and mechanical ventilation also cause iatrogenic pneumothorax, meaning one caused unintentionally by medical treatment.
Rib fractures account for the majority of blunt traumatic pneumothorax cases. Even without penetration, the force of impact can shear lung tissue or cause sudden pressure changes that rupture the pleura.
Tension Pneumothorax
Tension pneumothorax represents the most immediately life-threatening form. In this condition, a one-way valve mechanism allows air to enter the pleural space with each breath but prevents it from escaping. Pressure builds progressively inside the pleural cavity, collapsing the lung completely and pushing the heart and great vessels toward the opposite side of the chest, a finding called mediastinal shift.
This shift compresses the opposite lung and obstructs blood return to the heart, causing cardiovascular collapse within minutes. Tension pneumothorax constitutes a true medical emergency demanding immediate decompression without waiting for imaging confirmation.
Causes and Risk Factors for Pneumothorax
Several factors increase the likelihood of developing pneumothorax. Recognising these risk factors enables earlier vigilance and faster response.
Tall Stature and Body Habitus
Young, tall, lean males face the highest risk of primary spontaneous pneumothorax. Researchers believe that the relatively rapid growth of tall individuals causes uneven lung development, creating stress at the lung apex where blebs preferentially form. The exact mechanism remains incompletely understood, but the clinical association between tall stature and primary spontaneous pneumothorax is well established.
Marfan syndrome, a genetic connective tissue disorder characterised by tall stature and long limbs, carries a particularly elevated pneumothorax risk due to weakened lung tissue.
Smoking
Smoking significantly increases pneumothorax risk in both men and women. Tobacco smoke causes small airway inflammation, air trapping, and lung tissue damage that promotes bleb formation. Studies demonstrate a dose-dependent relationship between smoking intensity and pneumothorax risk, with heavy smokers facing dramatically higher rates than non-smokers.
Smoking cessation reduces but does not eliminate the elevated risk, particularly in those who smoked heavily during adolescence and early adulthood.
Underlying Lung Diseases
Several lung conditions directly predispose individuals to pneumothorax. COPD creates over-inflated, fragile lung tissue prone to rupture. Cystic fibrosis causes progressive airway damage and bleb formation. Pulmonary Langerhans cell histiocytosis, a rare inflammatory lung condition, carries an exceptionally high pneumothorax risk.
Lymphangioleiomyomatosis, a rare condition affecting predominantly women of reproductive age, causes cystic lung destruction and recurrent pneumothorax. Each of these conditions requires specific pneumothorax management strategies tailored to the underlying disease.
Mechanical Ventilation
People receiving mechanical ventilation in intensive care settings face elevated pneumothorax risk. High ventilator pressures can over-distend and rupture vulnerable lung tissue, causing barotrauma. Vigilant pressure monitoring and lung-protective ventilation strategies reduce but cannot entirely eliminate this risk.
Pneumothorax in a ventilated patient can escalate rapidly to tension pneumothorax given the continuous positive pressure being applied, requiring immediate clinical recognition.
Symptoms of Pneumothorax
Pneumothorax produces a recognisable symptom pattern, though severity varies considerably based on the size of the pneumothorax and the individual’s underlying lung health.
Sudden Chest Pain
Sharp, sudden chest pain on one side is the most characteristic symptom of pneumothorax. This pain typically begins abruptly, often during ordinary activity or even at rest, and worsens with breathing and movement. People frequently describe it as a stabbing or tearing sensation, distinct from the pressure or heaviness associated with cardiac chest pain.
The pain reflects stretching of the pleural membranes as air accumulates and the lung recoils. In some people, particularly those with small pneumothoraces, the pain gradually diminishes over hours even as the pneumothorax persists.
Breathlessness
Breathlessness accompanies chest pain in most pneumothorax cases. Its severity correlates broadly with pneumothorax size and the individual’s baseline lung function. A young, otherwise healthy person may experience only mild breathlessness from a moderate pneumothorax, while someone with severe underlying COPD can develop profound respiratory failure from even a small air leak.
Breathlessness in pneumothorax typically worsens with exertion and improves somewhat with rest, though it does not resolve until the air leak is addressed.
Signs of Tension Pneumothorax
Tension pneumothorax produces rapidly progressive symptoms. Extreme breathlessness, rapidly falling blood pressure, racing heart rate, distended neck veins, and tracheal deviation toward the opposite side of the chest all signal this emergency. Deteriorating consciousness and cardiovascular collapse follow quickly without immediate intervention.
Any person who develops rapidly worsening breathlessness and haemodynamic instability, particularly after chest trauma or during mechanical ventilation, requires immediate assessment for tension pneumothorax.
Atypical and Mild Presentations
Small pneumothoraces sometimes produce surprisingly mild symptoms. Some people experience only slight chest discomfort or notice mild breathlessness on exertion. Others present incidentally, with pneumothorax discovered on a chest X-ray performed for an unrelated reason. This symptom variability means clinicians must maintain a low threshold for investigating suspected pneumothorax even when symptoms seem minor.
Diagnosing Pneumothorax
Prompt and accurate diagnosis of pneumothorax guides appropriate treatment and prevents deterioration, particularly in tension pneumothorax where every minute matters.
Clinical Assessment
Experienced clinicians can identify pneumothorax through physical examination. On the affected side, breath sounds are reduced or absent when listening with a stethoscope, and percussion of the chest produces a hollow, drum-like resonance instead of the normal dull sound. The trachea, the main airway, may deviate toward the opposite side in large or tension pneumothorax.
In tension pneumothorax, clinical diagnosis should drive immediate treatment without waiting for imaging. The severity and speed of deterioration leave no time for confirmatory tests.
Chest X-Ray
Chest X-ray is the standard first-line imaging investigation for suspected pneumothorax in stable patients. On a plain chest X-ray, pneumothorax appears as a visible line separating the collapsed lung edge from the chest wall, with no lung markings visible beyond this line. The size of the pneumothorax is estimated based on the distance between the lung edge and chest wall.
Standard guidelines use this measured distance to classify pneumothorax as small or large, guiding treatment decisions.
CT Scanning
Computed tomography (CT) scanning of the chest provides the most detailed pneumothorax assessment. CT precisely measures pneumothorax size, identifies the site and nature of the air leak, detects underlying blebs or bullae, and reveals associated lung diseases. CT proves particularly valuable when chest X-ray findings are ambiguous or when planning surgical intervention.
CT also detects small pneumothoraces invisible on plain X-ray, which carries particular relevance in trauma patients where any pneumothorax can threaten stability if ventilation becomes necessary.
Ultrasound
Point-of-care chest ultrasound has become an important diagnostic tool, particularly in emergency medicine and intensive care. A trained clinician can identify pneumothorax within seconds using bedside ultrasound by detecting the absence of normal lung sliding movement against the chest wall. Ultrasound avoids radiation exposure and provides real-time assessment at the bedside.
In trauma settings, ultrasound integrated into the primary assessment detects pneumothorax rapidly and guides immediate management decisions.
Treatment of Pneumothorax
Treatment depends on pneumothorax type, size, symptoms, and underlying lung health. Options range from observation alone to emergency surgical intervention.
Conservative Management and Observation
Small primary spontaneous pneumothoraces in otherwise healthy people with minimal symptoms often resolve without active intervention. Air in the pleural space absorbs naturally over days to weeks as the body gradually reabsorbs the trapped gas. During this period, people require monitoring for symptom progression and repeat imaging to confirm resolution.
Activity restriction, avoidance of strenuous exertion, and clear instructions to return immediately if symptoms worsen accompany conservative management. Supplemental high-flow oxygen accelerates air reabsorption significantly and reduces resolution time.
Needle Aspiration
Needle aspiration offers a minimally invasive treatment for symptomatic primary spontaneous pneumothorax. A doctor inserts a needle or small cannula through the chest wall into the pleural space and withdraws the trapped air with a syringe. This procedure is straightforward, avoids hospitalisation in many cases, and carries low complication rates.
Success rates for needle aspiration range from 50 to 80 percent in primary spontaneous pneumothorax. Failed aspiration or recurrence after aspiration indicates the need for chest tube drainage.
Chest Tube Drainage
Chest tube insertion, also called tube thoracostomy, remains the most widely used active treatment for pneumothorax. A surgeon inserts a hollow tube through the chest wall into the pleural space under local anaesthesia. The tube connects to a drainage system that allows air to escape while preventing re-entry.
The tube remains in place until the air leak seals and the lung fully re-expands, typically over one to several days. Water seal drainage systems and suction can accelerate lung re-expansion in selected cases.
Emergency Needle Decompression
Tension pneumothorax demands immediate emergency needle decompression before any other intervention. A large-bore needle inserted through the second intercostal space at the midclavicular line releases the trapped pressurised air rapidly, decompressing the pleural cavity and restoring cardiac function. This life-saving manoeuvre converts the tension pneumothorax to an open pneumothorax that standard chest tube drainage can then manage definitively.
Failure to perform immediate needle decompression in tension pneumothorax results in rapid death. Pre-hospital responders, emergency physicians, and military medics all require proficiency in this procedure.
Surgical Treatment
Surgery addresses recurrent pneumothorax or cases where air leaks fail to seal with conservative measures. Video-assisted thoracoscopic surgery (VATS) allows surgeons to directly visualise the lung surface, staple off blebs and bullae responsible for air leaks, and perform pleurodesis.
Pleurodesis involves deliberately creating inflammation between the visceral and parietal pleura, causing them to fuse together. This fusion obliterates the pleural space, preventing future pneumothorax formation. Chemical pleurodesis using talc or tetracycline can be performed through a chest tube without surgery in selected cases.
Recurrence of Pneumothorax
Recurrence represents one of the most clinically important aspects of pneumothorax management, particularly after primary spontaneous pneumothorax.
Recurrence Rates
After a first primary spontaneous pneumothorax, recurrence rates reach approximately 30 to 50 percent without definitive treatment. Most recurrences happen within two years of the initial episode, with the first six months carrying the highest risk. Each subsequent pneumothorax increases the risk of further recurrences.
Smoking continuation, tall lean build, and the presence of multiple blebs on CT scanning all increase recurrence risk. These factors inform decisions about pursuing definitive surgical prevention after an initial episode.
Preventing Recurrence
VATS pleurodesis is highly effective at preventing recurrence, with success rates exceeding 95 percent. Surgical intervention becomes strongly recommended after a second ipsilateral pneumothorax, meaning a recurrence on the same side, or after a first contralateral pneumothorax, meaning one affecting the opposite lung. Certain occupations and activities including flying, diving, and remote fieldwork also justify early surgical prevention due to the life-threatening consequences of pneumothorax in these contexts.
Special Considerations in Pneumothorax
Certain groups and circumstances require tailored pneumothorax management approaches.
Pneumothorax in Pregnancy
Pneumothorax during pregnancy is uncommon but serious. The growing uterus limits respiratory reserve, making even moderate pneumothorax more symptomatic and dangerous. Management must balance maternal respiratory stability with fetal wellbeing. Multidisciplinary involvement of obstetricians, pulmonologists, and thoracic surgeons optimises outcomes for both the pregnant person and their baby.
Pneumothorax and Air Travel
Air travel creates particular risks for people with incompletely resolved pneumothorax. Cabin pressure at altitude is lower than at sea level, causing any residual trapped air to expand according to Boyle’s Law. This expansion can worsen a partially resolved pneumothorax into a symptomatic or even tension pneumothorax during flight.
Most guidelines recommend avoiding air travel until complete pneumothorax resolution, confirmed by imaging, has been achieved. People with a history of pneumothorax should discuss flight safety with their doctor before travelling.
Catamenial Pneumothorax
Catamenial pneumothorax is a rare but important condition affecting women of reproductive age. It occurs recurrently in association with menstrual periods, typically within 24 to 72 hours of menstrual onset. The underlying mechanism involves endometriosis, a condition where uterine lining tissue grows outside the uterus, including on or through the diaphragm and pleura.
Treatment involves hormonal therapy to suppress menstruation combined with surgical pleurodesis in recurrent cases.
Frequently Asked Questions
What causes pneumothorax?
Pneumothorax most commonly results from the spontaneous rupture of small blebs on the lung surface in otherwise healthy young people, or as a complication of underlying lung diseases such as COPD or cystic fibrosis. Chest trauma, medical procedures, and mechanical ventilation also cause pneumothorax. Smoking significantly increases bleb formation and pneumothorax risk, particularly in tall, lean individuals.
Is pneumothorax life-threatening?
Most pneumothoraces are not immediately life-threatening, particularly small primary spontaneous pneumothoraces in healthy young people. However, tension pneumothorax is a rapidly fatal emergency without immediate treatment. Secondary spontaneous pneumothorax in people with existing lung disease also carries significant mortality risk. Prompt recognition and appropriate management are essential in all cases.
Can pneumothorax heal on its own?
Small pneumothoraces in otherwise healthy people often resolve spontaneously as the body reabsorbs the trapped air over days to weeks. However, even small pneumothoraces require medical monitoring to confirm resolution and detect any expansion. Larger pneumothoraces, those in people with underlying lung disease, and all cases of tension pneumothorax require active medical intervention.
How long does recovery from pneumothorax take?
Recovery time depends on pneumothorax size, treatment approach, and underlying health. Small pneumothoraces managed conservatively typically resolve within one to two weeks. Larger ones requiring chest tube drainage usually resolve within several days of tube insertion. Full return to normal activities, including sport and strenuous exertion, generally takes four to six weeks after complete lung re-expansion.
Can pneumothorax come back?
Yes. Recurrence is common, particularly after primary spontaneous pneumothorax, with rates of 30 to 50 percent after a first episode. Smoking continuation, the presence of multiple lung blebs, and tall lean body habitus all increase recurrence risk. Surgical pleurodesis, usually performed via VATS, reduces recurrence risk to below five percent and is recommended after a second pneumothorax or in high-risk occupational contexts.
Can people with pneumothorax fly?
Flying is generally not safe until complete pneumothorax resolution is confirmed by imaging. Reduced cabin pressure at altitude causes trapped air to expand, potentially worsening a partially resolved pneumothorax. Most physicians recommend waiting until a follow-up chest X-ray or CT confirms full lung re-expansion before flying. People with a history of recurrent pneumothorax should seek medical advice before any air travel.
Disclaimer:
This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis, treatment, or medical guidance related to any health condition.
References:
- Thymoma is a tumor arising from thymic epithelial cells characterized by relatively indolent behavior, frequent myasthenia gravis association, and excellent prognosis in early-stage disease.
- Chest pain might seem like an obvious sign, but people often ignore it or blame it on other causes.
- Haemophilia A is an X-linked recessive genetic disorder caused by deficiency or dysfunction of clotting factor VIII.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.