
Morphea (Localized Scleroderma): The Skin-Hardening Condition Without Systemic Involvement
When skin suddenly becomes hard, discoloured, and thickened in patches, the experience can be alarming and confusing. Understanding what is happening and why transforms fear into actionable medical knowledge.
Morphea, also called localized scleroderma, is a rare inflammatory skin condition that causes patches of hardened, thickened skin due to excessive collagen deposition. Unlike systemic sclerosis, morphea confines its effects to the skin and immediately underlying tissues without damaging the internal organs, blood vessels, or lungs.
Despite being localised, morphea causes significant functional impairment, cosmetic distress, and in some subtypes, serious complications affecting joints and underlying structures. Recognising morphea localized scleroderma causes and seeking early specialist care prevents the most serious long-term consequences.
What Is Morphea?
Morphea is a chronic inflammatory skin disorder characterised by localised areas of skin fibrosis, meaning excessive collagen production that replaces normal skin with hardened, thickened tissue. The condition affects the dermis, the deeper layer of skin, and can extend into the subcutaneous fat, fascia, and even muscle and bone in severe forms.
The word “morphea” derives from the Greek word for form or shape, reflecting the well-circumscribed nature of the skin plaques. Individual lesions have a characteristic evolving appearance that progresses through distinct active and inactive phases.
How Morphea Differs From Systemic Sclerosis
Many people initially fear that morphea represents the skin manifestation of systemic sclerosis, a condition that causes life-threatening internal organ damage. However, these two conditions are fundamentally distinct despite sharing the feature of skin hardening.
Systemic sclerosis causes fibrosis in the lungs, kidneys, heart, and gastrointestinal tract alongside skin changes, and carries Raynaud’s phenomenon and specific autoantibodies as hallmark features. Morphea remains confined to the skin and underlying local structures, sparing internal organs entirely.
Who Develops Morphea?
Morphea affects people across all age groups, though it most commonly presents in adults between 40 and 50 years of age. A distinct paediatric form, particularly linear morphea, affects children and adolescents and requires especially careful management due to its potential to impair growth and joint function.
Women develop morphea approximately three times more often than men in adult populations. The condition affects all ethnicities and backgrounds, though certain subtypes show different frequency patterns across demographic groups.
Morphea Localized Scleroderma Causes: What Drives Skin Fibrosis?
The precise cause of morphea remains incompletely understood, though research has identified immune dysregulation and excessive fibroblast activation as central to the disease process. Fibroblasts are the skin cells responsible for producing collagen, the structural protein that gives skin its strength and flexibility.
In morphea, fibroblasts become abnormally activated and overproduce collagen at affected sites. This excessive collagen deposition replaces the normal flexible skin architecture with dense, hard fibrous tissue that restricts movement and alters skin appearance.
Autoimmune Mechanisms in Morphea
Morphea displays clear autoimmune characteristics despite not fitting neatly into classic autoimmune disease categories. Early morphea lesions show dense infiltrates of T lymphocytes and macrophages within the dermis, driving inflammation that subsequently activates fibroblasts.
Profibrotic cytokines including transforming growth factor-beta (TGF-β) and interleukin-4 play critical roles in sustaining fibroblast activation beyond the initial inflammatory phase. This sustained TGF-β signalling represents an important therapeutic target for future treatment development.
Genetic Susceptibility Factors
Genetic factors contribute to morphea susceptibility, with certain HLA alleles associating with increased disease risk. Family clustering of morphea and other autoimmune conditions occurs more frequently than chance would predict, suggesting shared genetic predisposition pathways.
However, morphea does not follow clear Mendelian inheritance patterns, indicating that multiple genes interact with environmental factors to determine individual disease risk. Twin studies and familial aggregation analyses continue to clarify the relative contributions of genetic and environmental factors.
Environmental and External Triggers
Several external triggers have been implicated in initiating morphea in susceptible individuals. Physical trauma to the skin, including surgery, injections, radiotherapy, and burns, can trigger morphea lesions at the injury site through mechanisms related to the Koebner phenomenon.
Infections including Borrelia burgdorferi, the bacterium causing Lyme disease, have been proposed as triggers in some geographic regions, though this association remains geographically variable and scientifically debated. Certain medications and vaccinations have also been reported as rare triggers in individual case reports.
Types of Morphea: A Clinical Classification
Morphea encompasses several clinically distinct subtypes that differ in their distribution, depth of tissue involvement, clinical behaviour, and potential for complications. Accurate subtype classification guides treatment selection and determines the intensity of monitoring required.
The most widely used classification system, developed by Laxer and Zulian, recognises five major subtypes: plaque morphea, linear morphea, generalised morphea, pansclerotic morphea, and mixed morphea. Each subtype carries distinct clinical implications.
Plaque Morphea: The Most Common Form
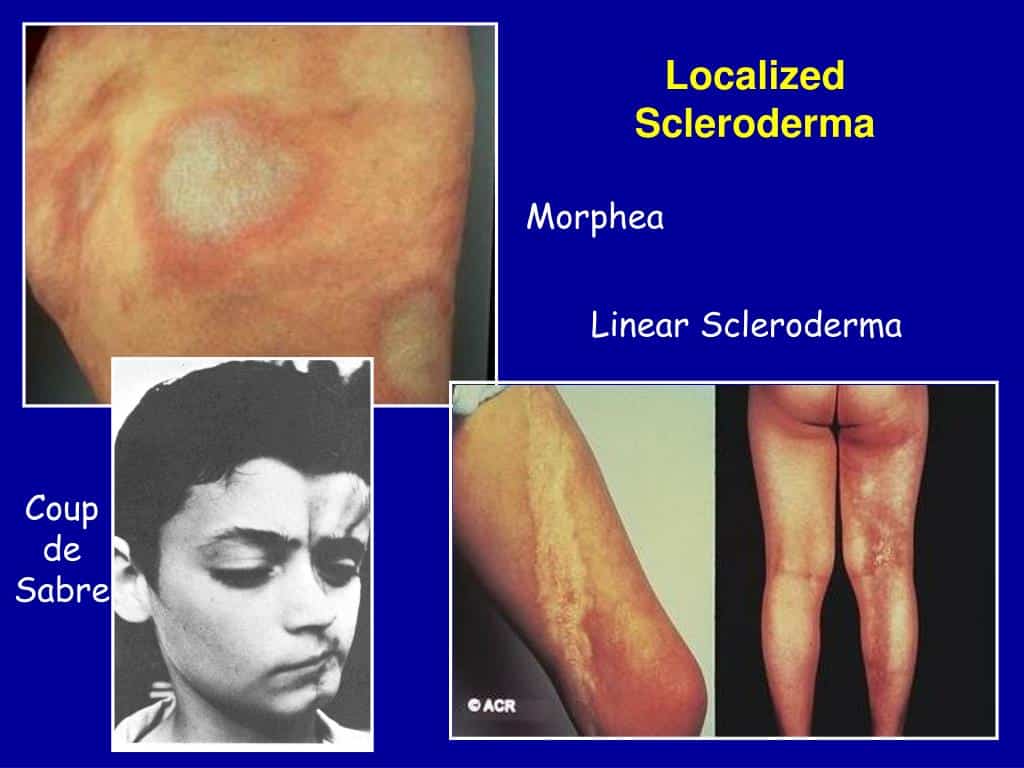
Plaque morphea is the most frequent adult subtype and presents as one or a few oval or round plaques on the trunk, limbs, or face. Active plaques display a characteristic appearance with a central area of ivory-white or yellowish hardened skin surrounded by a violaceous or lilac-coloured ring called the lilac ring or ring of lilac.
The lilac ring indicates active ongoing inflammation at the plaque periphery and signals that the lesion is still expanding. When this peripheral ring disappears, it indicates the plaque has entered an inactive or burned-out phase, though residual discolouration and skin changes may persist.
Linear Morphea and Its Special Significance
Linear morphea produces a streak or band of skin hardening that runs along a limb, the trunk, or the face and scalp in a linear distribution. This subtype is particularly common in children and adolescents and carries the greatest risk of serious functional complications.
When linear morphea crosses a joint, the fibrosis extending into underlying fascia, muscle, and periarticular structures can cause progressive joint contractures that permanently restrict movement. Early aggressive treatment aims to prevent this joint limitation before irreversible structural changes establish themselves.
En Coup de Sabre and Parry-Romberg Syndrome
En coup de sabre is a distinctive linear morphea variant affecting the frontoparietal scalp and face, producing a linear depression resembling the scar of a sabre blow. This visually striking subtype can cause scarring alopecia, dental abnormalities, and ocular complications.
Parry-Romberg syndrome, also called progressive facial hemiatrophy, represents the most severe facial linear morphea variant. It causes progressive atrophy of one side of the face affecting skin, fat, muscle, and sometimes underlying bone, producing significant and often progressive facial asymmetry.
Generalised and Pansclerotic Morphea
Generalised morphea involves four or more plaques distributed across two or more body regions, creating widespread skin hardening that can be functionally and cosmetically debilitating. Despite its extensive distribution, generalised morphea still confines itself to the skin and subcutaneous tissue without causing systemic organ involvement.
Pansclerotic morphea is the rarest and most severe subtype, causing circumferential skin hardening of the limbs that extends through all skin layers to involve fascia and muscle. This form can cause severe contractures, ulceration, and in rare cases has been associated with squamous cell carcinoma arising in chronic lesions.
Recognising the Symptoms of Morphea
Morphea lesions evolve through a predictable sequence of changes from initial inflammation through active fibrosis to eventual quiescence and residual discolouration. Recognising these stages helps clinicians assess disease activity and guide treatment timing effectively.
The earliest sign of a new morphea plaque is subtle erythema, meaning redness and mild swelling, at the affected skin site. Many patients also describe sensations of tightness, itching, or mild burning in the area before visible skin changes become apparent.
Active Phase Appearance
Active morphea plaques display the characteristic lilac ring surrounding a central area of indurated, meaning hardened, skin. The central skin feels firm or board-like when pressed, has lost its normal flexibility, and may appear ivory-white, yellowish, or waxy in colour.
Hair follicles and sweat glands within the plaque are progressively destroyed as fibrosis replaces normal skin architecture. This destruction of adnexal structures contributes to the smooth, hairless appearance of established morphea plaques and the loss of normal sweating function within affected areas.
Inactive Phase and Residual Changes
As morphea enters its inactive phase, the violaceous lilac ring fades and the central induration gradually softens over months to years. The remaining skin changes include persistent discolouration ranging from hyperpigmentation to hypopigmentation, permanent atrophy of skin and subcutaneous fat, and potential scarring.
Residual skin changes persist after the active disease process subsides, representing the accumulated structural damage from the fibrotic process. The extent of permanent change depends heavily on the subtype, duration of active disease, depth of tissue involvement, and adequacy of treatment during the active phase.
Functional Impairment in Linear Morphea
Linear morphea crossing joints causes the most functionally significant symptoms of any morphea subtype. Progressive tightening of skin and deeper tissues limits joint range of motion, producing contractures that impair daily activities, walking, and upper limb function.
Children with linear morphea affecting a growing limb may experience limb length discrepancy as fibrosis impairs normal tissue growth on the affected side. Regular physiotherapy, aggressive early anti-inflammatory treatment, and close growth monitoring are all essential components of management in paediatric linear morphea.
Diagnosing Morphea Accurately
Accurate morphea diagnosis requires combining clinical assessment with appropriate investigations to confirm the diagnosis, classify the subtype, and exclude systemic sclerosis. The clinical appearance of characteristic morphea lesions allows experienced dermatologists to make a presumptive diagnosis in straightforward cases.
However, several other skin conditions including lichen sclerosus, radiation-induced skin fibrosis, eosinophilic fasciitis, and early systemic sclerosis can produce skin hardening that mimics morphea, making confirmation important in atypical cases.
Skin Biopsy Findings
A skin biopsy from an active morphea plaque provides histopathological confirmation of the diagnosis. Early biopsy specimens show dense perivascular lymphocytic inflammation in the deep dermis alongside early collagen thickening and the swelling of collagen bundles.
Established morphea shows dense, homogenised, eosinophilic collagen bundles replacing the normal reticular dermis, loss of adnexal structures, and a sparse inflammatory infiltrate. These characteristic histopathological features distinguish morphea from other fibrosing skin conditions with reasonable diagnostic confidence.
Blood Tests and Autoantibody Screening
Antinuclear antibody (ANA) testing returns positive in approximately 40 to 60% of morphea patients. Anti-single-stranded DNA antibodies and anti-histone antibodies associate more specifically with morphea than with systemic sclerosis.
Importantly, the scleroderma-specific antibodies including anti-topoisomerase I (anti-Scl-70) and anti-centromere antibodies, which characterise systemic sclerosis, are absent in morphea. This negative antibody profile, combined with the absence of Raynaud’s phenomenon and normal nailfold capillaroscopy, effectively distinguishes morphea from systemic sclerosis.
Imaging in Linear Morphea
Magnetic resonance imaging (MRI) proves particularly valuable in linear morphea to assess the extent of deep tissue involvement beyond the visible skin changes. MRI clearly delineates fascial, muscular, periarticular, and in craniofacial cases, intracranial involvement that clinical examination cannot adequately visualise.
Ultrasound imaging assesses skin thickness and dermal echogenicity non-invasively, providing a radiation-free tool for monitoring disease activity and treatment response over time. Serial ultrasound measurements document skin softening during treatment in a quantifiable way.
Treating Morphea: Matching Therapy to Disease Severity
Morphea treatment follows a principle of matching therapeutic intensity to disease severity, subtype, and activity level. Inactive or mildly active plaque morphea in a cosmetically non-sensitive location may require only emollient care and sun protection.
Active, progressive, or functionally threatening morphea requires prompt initiation of disease-modifying treatment to prevent irreversible damage during the active fibrotic phase. Specialist dermatology and, for paediatric linear cases, paediatric rheumatology input guide treatment decisions.
Topical and Local Treatments
High-potency topical corticosteroids reduce inflammation in early, superficial morphea plaques and provide a useful first-line option for mild, localised disease. Topical calcipotriol and calcitriol, vitamin D analogues, exert antifibrotic effects and show modest benefit for limited plaque morphea in clinical studies.
Imiquimod cream, an immune response modifier, has demonstrated efficacy in small morphea studies by modulating the profibrotic cytokine environment within active lesions. Topical tacrolimus provides an additional steroid-free anti-inflammatory option, particularly for facial or sensitive-site morphea.
Phototherapy for Active Morphea
Ultraviolet A1 (UVA1) phototherapy is the most evidence-supported light-based treatment for active morphea. High-dose UVA1 penetrates deep into the dermis, inducing collagenase activity that breaks down the excess collagen deposited during the fibrotic process.
Multiple clinical trials demonstrate significant skin softening and reduction in morphea clinical scores following UVA1 phototherapy courses. Narrowband UVB phototherapy provides an alternative with good availability in phototherapy centres, though its evidence base for morphea is less extensive than UVA1.
Systemic Treatments for Severe or Progressive Morphea
Methotrexate is the most widely used and best-evidenced systemic treatment for severe or rapidly progressive morphea, particularly linear and generalised subtypes. Weekly low-dose methotrexate suppresses the T cell-driven inflammatory phase and reduces profibrotic cytokine production that activates fibroblasts.
Combination therapy with oral corticosteroids during the initial three to six months accelerates the onset of disease control while methotrexate reaches therapeutic effect. Most treatment guidelines recommend continuing methotrexate for at least two to three years to prevent relapse after achieving clinical remission.
Mycophenolate Mofetil and Other Agents
Mycophenolate mofetil serves as an alternative systemic immunosuppressant for patients who cannot tolerate methotrexate or respond inadequately to it. Clinical series report meaningful improvements in morphea activity scores with mycophenolate therapy, and it is increasingly used as both a primary and rescue treatment option.
Hydroxychloroquine, abatacept, and several other immunomodulatory agents have been explored in small morphea cohorts with variable results. Anti-fibrotic agents including nintedanib and pirfenidone represent emerging treatment possibilities based on their established efficacy in other fibrosing conditions.
Physiotherapy and Rehabilitation in Morphea
Physical and occupational therapy form essential components of morphea management, particularly for linear subtypes with functional implications. No medication alone can restore joint range of motion once contractures establish themselves, making active rehabilitation indispensable alongside systemic treatment.
Regular stretching exercises targeting affected joints prevent progressive loss of movement during active disease and maintain gains achieved during treatment. Physiotherapists experienced with inflammatory skin and connective tissue conditions provide individually tailored exercise programmes based on the specific joints and body areas affected.
Splinting and Orthotics
Custom-made splints hold affected joints in positions of optimal function during rest, counteracting the fibrotic forces that pull joints into contracture. Serial splinting progressively improves joint positioning as treatment softens the affected tissues over time.
Orthotics support affected limbs, improve gait biomechanics in lower limb linear morphea, and reduce the compensatory strain on unaffected joints. Early orthotic provision prevents secondary musculoskeletal problems that develop when people adapt their movement patterns to accommodate fibrosis-restricted joints.
Psychological Support and Quality of Life
The psychological burden of morphea, particularly visible facial and linear subtypes, significantly affects quality of life, self-esteem, and social participation. Children with linear en coup de sabre and adults with facial plaque morphea face particular challenges related to the visibility of their condition.
Psychological support, peer group connections through patient advocacy organisations, and age-appropriate educational support for affected children all address dimensions of morphea care that dermatological treatment alone cannot resolve. Holistic management acknowledges and actively addresses the full human impact of this chronic condition.
Frequently Asked Questions About Morphea
What causes morphea localized scleroderma to develop?
Morphea develops through a combination of immune dysregulation, excessive fibroblast activation, and overproduction of collagen in the affected skin areas. T lymphocytes and profibrotic cytokines, particularly TGF-β, drive the fibrotic process in genetically susceptible individuals. Environmental triggers including physical skin trauma, radiation, and possibly certain infections can initiate disease in predisposed people, though the precise cause remains incompletely understood in most individual cases.
Does morphea ever affect internal organs?
Morphea remains confined to the skin, subcutaneous tissue, and in severe subtypes, deeper local structures such as fascia and muscle. It does not affect the lungs, kidneys, heart, or gastrointestinal tract, distinguishing it clearly from systemic sclerosis which causes serious internal organ damage. However, approximately 5 to 10% of people with morphea have other associated autoimmune conditions, and those with generalised disease should receive periodic monitoring to detect any unexpected systemic features.
Can morphea go away without treatment?
Plaque morphea in adults often undergoes spontaneous partial resolution over three to five years as the active inflammatory phase burns out and leaves behind residual pigment changes and variable degrees of skin softening. However, linear morphea in children rarely resolves adequately without treatment and causes progressive joint contractures and growth disturbances when left untreated. Active treatment during the inflammatory phase reduces permanent skin damage, preserves joint function, and improves long-term cosmetic and functional outcomes across all subtypes.
What is the difference between morphea and systemic sclerosis?
Morphea and systemic sclerosis both cause skin hardening through collagen overproduction but are fundamentally different diseases with distinct mechanisms and prognoses. Morphea confines its effects to the skin and local structures without causing internal organ fibrosis or Raynaud’s phenomenon. Systemic sclerosis causes progressive fibrosis of the lungs, kidneys, heart, and gastrointestinal tract alongside skin changes and carries specific autoantibodies including anti-centromere and anti-Scl-70 that are absent in morphea.
How effective is methotrexate for treating morphea?
Methotrexate is the most evidence-supported systemic treatment for severe or rapidly progressive morphea, particularly linear and generalised subtypes. Clinical studies and expert guidelines consistently support its use as first-line systemic therapy, with most patients showing meaningful improvement in skin softening and reduction in disease activity scores over six to twelve months of treatment. Combining methotrexate with initial corticosteroids achieves faster disease control, and continuing methotrexate for two to three years reduces the risk of relapse after achieving remission.
Early Treatment of Morphea Prevents a Lifetime of Unnecessary Impairment
Morphea may not threaten life the way systemic diseases do, but it can permanently alter skin structure, restrict joint movement, impair growth, and profoundly affect quality of life when it progresses without adequate treatment.
Modern dermatology and rheumatology offer effective therapeutic tools capable of halting active fibrosis, softening established skin changes, and preserving functional capacity when treatment begins during the active inflammatory phase. From UVA1 phototherapy to methotrexate and emerging antifibrotic agents, the treatment landscape continues to evolve.
Most importantly, no person with morphea should accept progressive skin hardening and functional loss as inevitable. Early specialist diagnosis, appropriate subtype classification, timely systemic treatment, and integrated physiotherapy together provide the best possible defence against the permanent consequences this condition otherwise inflicts.
Disclaimer:
This article is intended for general informational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for any medical concerns.
References:
- Systemic Sclerosis, commonly called Scleroderma, is a chronic autoimmune disease characterized by progressive fibrosis of skin and internal organs.
- Systemic sclerosis is a chronic autoimmune connective tissue disease characterized by skin fibrosis and often involving internal organs.
- Psoriasis is a chronic autoimmune inflammatory disease that affects the skin, and often affects other organs and body systems.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.