
Dupuytren’s Contracture: The Viking Disease Explained
The hand is one of the most precisely engineered structures in the body. It grasps, pinches, types, and performs tasks of extraordinary delicacy. However, for some people, a slow and invisible process begins beneath the skin of the palm. It gradually pulls one or more fingers into a bent position from which they cannot straighten.
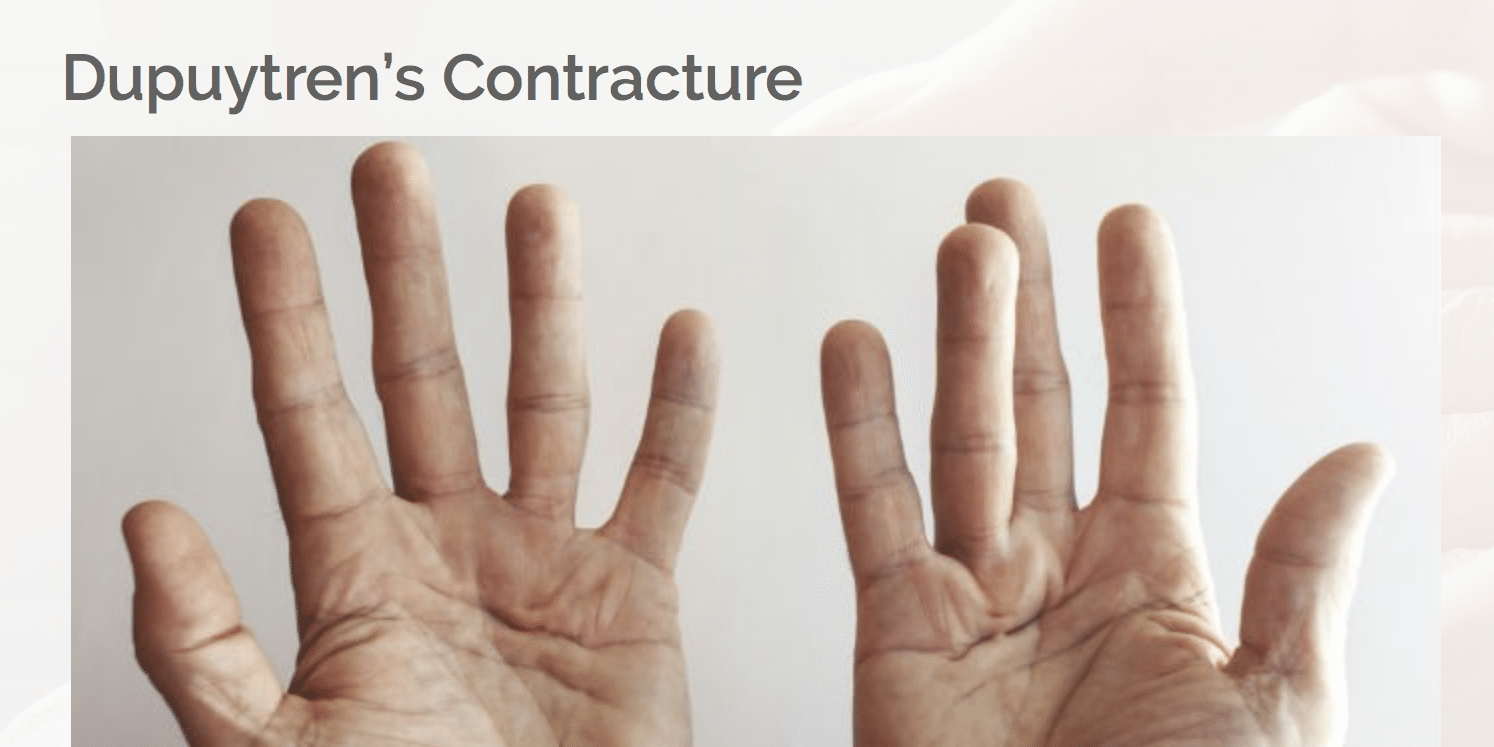
Dupuytren’s contracture is a condition in which connective tissue beneath the palm thickens and forms rope-like cords. These cords pull the fingers — most often the ring and little fingers — into a permanent flexed position. Over time, gripping, handshaking, and washing the face all become difficult or impossible.
Dupuytren’s contracture Viking disease curls fingers is more than a historical nickname. It reflects a genuine epidemiological pattern — the condition is most common in people of northern European ancestry. Furthermore, it affects men far more than women and becomes increasingly common with age. Consequently, understanding what causes it and what modern medicine can do to straighten the fingers gives patients the information they need to act at the right time.
Quick Answer
Dupuytren’s contracture is a progressive hand condition. Thickened cords of connective tissue under the palm pull the fingers — most commonly the ring and little fingers — into a permanently bent position. It develops slowly over years and is more common in men of northern European descent. Treatment includes needle fasciotomy, collagenase injection, or surgery.
What Is Dupuytren’s Contracture?
The Palmar Fascia and What Goes Wrong
Beneath the skin of the palm lies a thin layer of connective tissue called the palmar fascia. This fibrous layer anchors skin to underlying bones and tendons. It also helps distribute grip forces evenly across the palm. In healthy hands, this layer is flat, flexible, and largely invisible.
In Dupuytren’s contracture, specialised cells called myofibroblasts become abnormally active. These cells produce excessive amounts of collagen — the protein that forms connective tissue. As a result, they deposit firm nodules — pea-sized lumps — within the palmar fascia. Over time, these nodules extend into rope-like cords running toward the fingers. Furthermore, these cords contract and pull the affected fingers steadily toward the palm.
How the Disease Progresses
Dupuytren’s contracture typically progresses slowly over years. The first sign is usually a small, firm nodule near the base of the ring or little finger. The overlying skin may dimple or pucker as the thickening fascia pulls it from beneath.
Over months to years, cords extend from the nodule toward the finger. They cross the knuckle joint and attach to the bone and tendon sheath. As the cord tightens, the finger bends progressively toward the palm. Consequently, the degree of contracture — the angle at which the finger stays bent — increases over time without treatment. For context on how progressive connective tissue conditions affect daily life, see our article on fibromyalgia — the pain condition that is real, widely misunderstood, and treatable.
Why Is It Called the Viking Disease?
Geographic and Ancestral Patterns
Dupuytren’s contracture Viking disease curls fingers reflects a well-documented prevalence pattern. The condition is most common in people of northern European ancestry — particularly those from Norway, Iceland, Scotland, Ireland, and the Netherlands. In some Scandinavian populations, prevalence reaches 30% in adults over 60. In contrast, it is extremely rare in people of Asian, African, and Middle Eastern ancestry.
Researchers attribute this distribution to genetic variants carried by northern European populations. Historical Norse migrations across the North Sea into Britain, Ireland, and Iceland likely spread these variants widely. Consequently, the nickname Viking disease has become widely used in medical literature and popular culture.
However, the label oversimplifies a complex genetic and environmental picture. Moreover, not everyone with Dupuytren’s contracture has Viking ancestry — the condition occurs across many populations at lower rates. Consequently, the nickname is a useful memory aid rather than a complete epidemiological explanation.
The Role of Genetics
Genetics plays a central role in Dupuytren’s contracture. The condition runs strongly in families — first-degree relatives of affected individuals face a significantly elevated lifetime risk. Furthermore, research has identified multiple genetic variants associated with the condition. These variants affect fibroblast activity, collagen metabolism, and the Wnt signalling pathway — a molecular system that regulates cell growth.
Having a strong genetic predisposition does not guarantee the condition will develop or become severe. Environmental and lifestyle factors modify genetic risk significantly. Consequently, understanding which factors worsen the condition gives patients meaningful opportunities to influence their own disease course.
Risk Factors and Causes
Who Is Most at Risk?
Dupuytren’s contracture becomes increasingly common with advancing age. It is rare before 40 but affects roughly 20% of men over 65 in northern European populations. Furthermore, men develop the condition five to ten times more frequently than women. Women who develop it typically do so a decade or more later in life, often with milder progression.
Diabetes significantly increases risk. People with diabetes — particularly those with long-standing or poorly controlled disease — develop the condition at higher rates. Moreover, epilepsy and the anticonvulsant medications used to treat it have historically been associated with elevated Dupuytren’s risk, though the precise mechanism remains under investigation.
Lifestyle and Occupational Factors
Heavy alcohol consumption increases Dupuytren’s contracture risk. The likely mechanism involves alcohol-induced liver disease, which alters the metabolism of growth factors that regulate fibroblast activity. In addition, smoking significantly elevates risk — possibly through vascular effects on palmar circulation or direct effects on fibroblast behaviour.
Vibrating hand tool use — common in construction, forestry, and engineering — is associated with increased risk in some studies. Consequently, occupational health monitoring for workers with prolonged vibration exposure is recommended in some countries. However, repetitive hand use without vibration exposure does not clearly increase risk on current evidence. For context on other musculoskeletal conditions affecting hand and shoulder function, see our article on rotator cuff tear — symptoms, diagnosis, and when surgery is actually needed.
Symptoms of Dupuytren’s Contracture
Early Signs
The earliest symptom is typically a small, firm nodule in the palm near the base of the ring or little finger. This nodule may feel slightly tender when pressed. Furthermore, the overlying skin sometimes dimples or puckers — a visible sign that tethering is occurring beneath the surface.
At this stage, the condition causes no functional limitation. Finger movement remains full and unrestricted. Consequently, many people discover the condition incidentally — feeling the nodule by chance or having it noted during a routine medical examination. However, early recognition is valuable because it allows monitoring and timely treatment planning before significant contracture develops.
Progressive Contracture and Functional Limits
As cords develop and extend toward the fingers, progressive contracture follows. The ring finger is most commonly affected, followed by the little finger. The middle finger, index finger, and thumb are less frequently involved. Furthermore, both hands are affected in roughly half of all patients — though typically not simultaneously.
The metacarpophalangeal joint — the large knuckle at the finger base — usually contracts first. Later, the proximal interphalangeal joint — the middle knuckle — becomes involved. Contracture at this middle knuckle is particularly problematic. It is more difficult to correct fully and more prone to recurrence after treatment. Consequently, seeking treatment before significant middle knuckle contracture develops improves outcomes significantly.
Daily Life Impact
Functional limitations develop progressively as contracture increases. People cannot place the hand flat on a table — a clinical sign called the table-top test — when contracture exceeds roughly 30 degrees at the base knuckle. Handshaking becomes awkward. Glove wearing, keyboard typing, and handling small objects all become increasingly difficult.
Moreover, washing the face and reaching into pockets become restricted in severe cases. Consequently, the impact on daily independence can become significant before many patients seek medical help. For context on managing other progressive joint and musculoskeletal conditions, see our article on osteoarthritis — inflammation, causes, and what actually helps.
How Doctors Diagnose Dupuytren’s Contracture
Clinical Assessment
Dupuytren’s contracture receives its diagnosis clinically — meaning physical examination alone provides sufficient information in most cases. No blood tests or imaging studies are routinely required.
The hand surgeon examines the palm and fingers for nodules, skin pits, and palpable cords running toward the fingers. Furthermore, doctors measure the degree of contracture at each affected joint using a goniometer — a simple protractor-like measuring tool — to quantify functional limitation precisely. The table-top test quickly screens for significant contracture.
Assessing Dupuytren’s Diathesis
Dupuytren’s diathesis refers to a particularly aggressive disease pattern that predicts faster progression and higher recurrence risk after treatment. Surgeons assess for specific features that indicate diathesis.
These features include early age of onset — before 50 — bilateral hand involvement, and ectopic lesions — nodules occurring outside the palm. Ectopic sites include the knuckle pads of the fingers called Garrod’s pads, the soles of the feet in a condition called Ledderhose disease, and the penis in a condition called Peyronie’s disease. Consequently, identifying diathesis features helps surgeons counsel patients realistically about recurrence likelihood after treatment.
When Imaging Is Used
Ultrasound provides useful preoperative information in complex cases. It maps cord extent, identifies the proximity of digital nerves and arteries, and detects disease in areas not easily palpable. MRI is occasionally used in recurrent disease — particularly when previous surgery has created scar tissue that distorts normal anatomy.
Consequently, imaging supplements rather than replaces thorough clinical assessment in Dupuytren’s contracture. Moreover, most patients proceed directly from clinical examination to treatment planning without any imaging.
Treatment of Dupuytren’s Contracture
Watchful Waiting
Not all Dupuytren’s contracture requires immediate treatment. Nodules without significant contracture — particularly in older adults with slow-progressing disease — can be safely monitored. Doctors advise annual review and ask patients to return promptly if contracture progresses beyond 30 degrees at the base knuckle.
The table-top test provides a simple self-monitoring tool. Patients check regularly whether the affected hand lies flat on a firm surface. When the hand no longer flattens, the threshold for treatment has typically been reached. Consequently, self-monitoring allows timely intervention before severe contracture makes treatment more difficult.
Needle Fasciotomy
Needle fasciotomy — also called percutaneous needle aponeurotomy — is a minimally invasive procedure. A surgeon inserts a hypodermic needle through the skin to perforate and divide the contracting cord at multiple points. Once weakened, the cord ruptures when the finger is straightened. Furthermore, the procedure takes roughly 30 minutes per finger and requires no incision or stitches.
Most patients return to full hand use within days. Moreover, the procedure takes place in an outpatient clinic without general anaesthesia. However, recurrence rates are higher than after surgical removal of the cord. Consequently, needle fasciotomy suits older patients with milder contracture or those who need rapid return to function.
Collagenase Injection
Collagenase clostridium histolyticum — marketed as Xiaflex — is an enzyme derived from bacteria. It dissolves collagen when injected directly into the Dupuytren’s cord. Over 24 to 72 hours, the enzyme breaks down the cord’s collagen fibres. The surgeon then firmly manipulates the finger to rupture the weakened cord and straighten it.
The entire treatment involves just two outpatient clinic visits separated by two days. Furthermore, no surgery is required. Collagenase achieves excellent correction of base knuckle contracture in the majority of patients. However, it is less effective for middle knuckle contracture and carries higher recurrence rates than surgical removal. Consequently, collagenase injection is best suited to appropriately selected patients where regulatory access is available.
Surgical Fasciectomy
Surgical fasciectomy involves the open surgical removal of the diseased palmar fascia and cords. The surgeon makes a zigzag incision across the palm and affected finger. This zigzag pattern prevents scar contracture across the skin during healing. The surgeon then carefully dissects the thickened cords away from the underlying digital nerves, arteries, and tendons.
Limited fasciectomy removes only the diseased tissue. It is the most commonly performed procedure. Radical fasciectomy removes all palmar fascia including normal tissue. However, it carries higher complication rates and is rarely performed today. Furthermore, dermofasciectomy — removing the overlying skin together with the cords and replacing it with a skin graft — is reserved for severe recurrent cases.
Post-Surgical Rehabilitation
Recovery after surgical fasciectomy involves a splint for two to four weeks. Hand physiotherapy then restores movement and prevents secondary stiffness. Night splinting continues for several months afterward. It prevents scar tissue from contracting the finger back into flexion during healing.
Physiotherapy compliance after surgery is as important as the surgical technique itself. Consequently, patients must commit fully to their rehabilitation programme to achieve the best long-term outcome. For context on rehabilitation after upper limb procedures, see our article on osteoarthritis — inflammation, causes, and what actually helps.
Living Well With Dupuytren’s Contracture
After Treatment
Most patients achieve significant improvement in finger extension after treatment — regardless of method chosen. However, recurrence is a reality for many patients — particularly those with Dupuytren’s diathesis. Recurrence rates at five years range from roughly 50% after needle fasciotomy and collagenase injection to 20 to 40% after surgical fasciectomy.
Regular review after treatment monitors for recurrence. It also allows timely re-treatment before contracture becomes severe again. Furthermore, many patients require sequential treatments over their lifetime. Consequently, Dupuytren’s contracture management is best understood as a long-term relationship between patient and hand specialist.
Lifestyle Adjustments
Addressing modifiable risk factors reduces progression and recurrence rates. Stopping smoking and significantly reducing alcohol intake remove two important drivers of fibroblast activity. Moreover, tight blood sugar control in people with diabetes reduces the risk of multi-digit involvement.
Hand stretching exercises do not prevent cord formation. However, they maintain joint flexibility and help monitor contracture development over time. For context on managing progressive musculoskeletal conditions requiring long-term monitoring, see our articles on spondylolisthesis — slipped vertebra, back pain, and treatment — and osteoporosis — how bones lose density and what reverses it.
When to Seek Medical Help
See a hand surgeon when a nodule has progressed to a palpable cord, when a finger cannot lay flat on a table, or when contracture exceeds 30 degrees at any joint. Furthermore, seek earlier assessment if both hands are involved, disease progresses rapidly, or nodules develop on the knuckle pads, soles of the feet, or in the penis.
Consequently, early referral to a specialist hand surgery unit gives patients access to the full range of treatment options before severe contracture makes correction technically more challenging.
Frequently Asked Questions
1. Is Dupuytren’s contracture painful?
Dupuytren’s contracture is not typically painful in most patients — particularly in the later stages when cords are established. The initial nodules can be tender when pressed during the early inflammatory phase. However, the progressive contracture itself is painless in the majority of cases. Consequently, the principal impact is functional — the inability to straighten the fingers — rather than pain. Significant ongoing pain should prompt assessment for coexisting conditions such as trigger finger or arthritis.
2. Does Dupuytren’s contracture affect only men?
No, but men develop the condition far more frequently — roughly five to ten times more often than women. Furthermore, women who develop Dupuytren’s contracture typically do so at an older age and often experience slower progression. Consequently, while the condition predominantly affects older men of northern European ancestry, women and individuals of other ancestries can develop it and deserve equal access to diagnosis and treatment.
3. Can Dupuytren’s contracture affect fingers other than the ring and little finger?
Yes. While the ring and little fingers are most commonly affected, Dupuytren’s contracture can involve any finger — including the middle finger, index finger, and occasionally the thumb. Furthermore, in people with Dupuytren’s diathesis, multiple fingers across both hands can develop contracture simultaneously. Consequently, any thickening or pitting in the palm or progressive flexion of any finger deserves specialist assessment.
4. Will Dupuytren’s contracture always get worse without treatment?
Not necessarily. Some patients develop a nodule that remains stable for many years without progressing to significant contracture. Others progress rapidly. The rate varies enormously between individuals and correlates with the presence or absence of diathesis features. Furthermore, age at onset, family history, and multiple finger involvement all influence the likelihood of progression. Consequently, regular monitoring rather than immediate treatment is entirely appropriate for mild or slowly progressing disease in older patients with low functional demands.
5. Is there any way to prevent Dupuytren’s contracture?
There is no proven way to prevent Dupuytren’s contracture in genetically susceptible individuals. However, stopping smoking, reducing alcohol intake significantly, and optimising blood sugar control in people with diabetes all reduce the risk of disease progression and severity. Furthermore, people with a strong family history benefit from knowing the early signs — nodules, skin pitting, and progressive finger bending — so they can seek treatment promptly. Consequently, awareness and early specialist referral represent the most practical preventive strategies currently available.
References
- Cerebral palsy is a group of permanent movement and posture disorders caused by abnormal brain development or brain damage occurring in the perinatal period.
- Systemic Sclerosis causes progressive symptoms affecting skin and potentially multiple organ systems.
- Dermatomyositis is a chronic autoimmune inflammatory disease affecting both muscles and skin simultaneously.
Disclaimer
This article adapts publicly available information from WHO’s Musculoskeletal Conditions page. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform and not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.