
Avascular Necrosis: When Bone Dies From Lack of Blood
Every living tissue in the body depends on a steady supply of blood. Blood delivers oxygen and nutrients that keep cells alive. When that supply is cut off — even temporarily — cells begin to die. Most tissues can recover from brief interruptions. However, bone tissue is far less forgiving.
Avascular necrosis — also called osteonecrosis — is a condition in which bone tissue dies because its blood supply is cut off or severely reduced. Without blood, bone cells stop functioning and begin to collapse from within. The affected bone gradually weakens, loses its structural integrity, and eventually crumbles — destroying the joint it supports. The hip is the most commonly affected site, though the condition can damage any bone in the body.
Avascular necrosis bone tissue dies blood supply is a condition that strikes people of all ages — including young adults in their twenties and thirties. Furthermore, it often develops silently in its early stages, causing no pain until significant bone damage has already occurred. Consequently, understanding what causes avascular necrosis, how to recognise it, and when to seek treatment is essential — because catching this condition early can mean the difference between saving a joint and replacing it entirely.
Quick Answer
Avascular necrosis — also called osteonecrosis — is a condition in which bone tissue dies due to loss of blood supply. It most commonly affects the hip joint. Causes include steroid use, alcohol, trauma, and blood disorders. Early diagnosis allows joint-preserving treatments. Advanced disease typically requires joint replacement surgery.
What Is Avascular Necrosis?
How Bone Depends on Blood Supply
Bone is living tissue that requires a constant supply of blood to survive. The network of blood vessels running through and around bone tissue delivers oxygen, removes waste products, and brings the raw materials bone cells need to rebuild and repair themselves. Bone cells — called osteocytes — die within hours when their blood supply is interrupted.
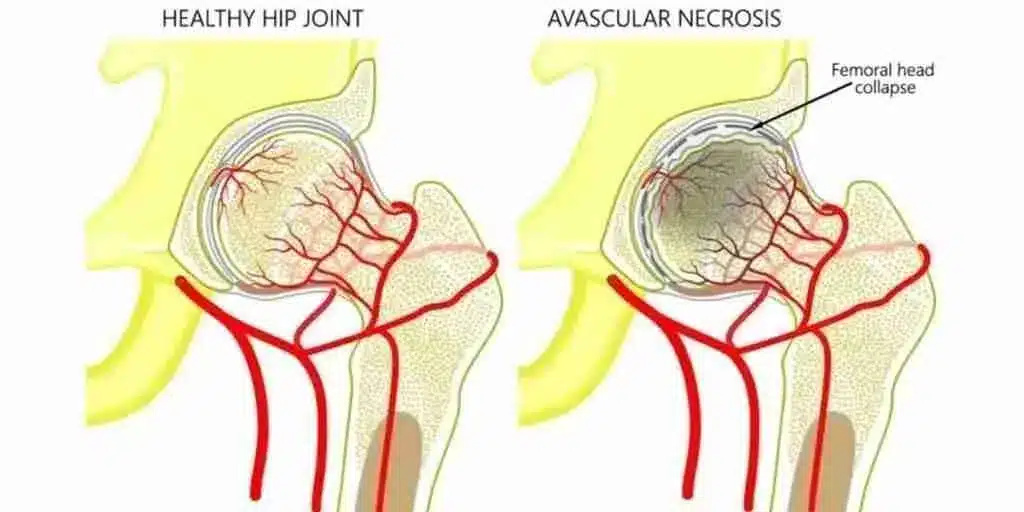
Unlike muscle tissue, which has rich redundant blood supply from multiple directions, certain bones — particularly the rounded head of the femur, which forms the ball part of the hip joint — receive blood through only a small number of vessels. Consequently, when even one or two of these critical vessels are blocked, damaged, or compressed, the bone loses its lifeline and begins to die.
What Happens as Bone Dies
The process of avascular necrosis bone tissue dies blood supply follows a predictable sequence if the underlying problem goes untreated. Initially, bone cells in the affected area die silently — producing no symptoms and no visible changes on standard X-ray. As the bone weakens progressively, microfractures form within the dying tissue. The structural support beneath the joint surface crumbles. Finally, the surface of the bone collapses — a catastrophic event that destroys the smooth joint surface and leads rapidly to severe arthritis.
This progression from silent bone death to joint collapse can occur over months to a few years. Moreover, the speed of progression depends on the size of the affected area, the underlying cause, and whether the cause has been removed. For broader context on how bone health conditions develop and are managed, see our article on osteoporosis — how bones lose density and what reverses it.
Causes of Avascular Necrosis
Corticosteroid Use
Corticosteroid medications — often called steroids — are the most common non-traumatic cause of avascular necrosis worldwide. Doctors prescribe corticosteroids for a wide range of conditions including asthma, rheumatoid arthritis, lupus, inflammatory bowel disease, and organ transplant rejection. However, prolonged use or high doses of corticosteroids significantly increase the risk of osteonecrosis.
Researchers believe corticosteroids cause osteonecrosis through two main mechanisms. First, they promote fat cell enlargement inside bone marrow — increasing pressure within the bone and compressing the internal blood vessels. Second, they directly damage the walls of small blood vessels supplying bone tissue, reducing blood flow. Consequently, the risk of avascular necrosis rises with higher steroid doses and longer treatment durations. For context on autoimmune conditions requiring long-term steroid treatment, see our article on lupus nephritis — when lupus attacks the kidneys.
Alcohol and Trauma
Heavy and prolonged alcohol use is the second most common cause of non-traumatic avascular necrosis. Alcohol promotes fat accumulation in the bloodstream — a condition called fat embolism — where fat droplets block the small vessels supplying bone tissue. Furthermore, alcohol interferes directly with bone cell function and bone marrow fat metabolism. Consequently, people who consume large amounts of alcohol regularly face a substantially elevated risk of developing osteonecrosis.
Trauma — including fractures, dislocations, and significant joint injuries — is the most common cause of avascular necrosis in younger people. A hip dislocation or femoral neck fracture can tear or compress the small blood vessels supplying the femoral head — the ball part of the hip joint — directly and immediately. Moreover, the risk of post-traumatic osteonecrosis increases with the severity of the injury and the time between injury and surgical repair.
Blood Disorders and Other Causes
Several blood disorders directly impair blood flow to bone tissue. Sickle cell disease — an inherited condition in which red blood cells become misshapen — causes these abnormal cells to clump together and block small blood vessels throughout the body, including those supplying bone. Consequently, sickle cell disease is one of the most common causes of avascular necrosis in younger patients and can affect multiple bones simultaneously.
Other causes include Gaucher disease — a metabolic storage disorder — radiation therapy to bones, decompression sickness in deep-sea divers — also called the bends — certain clotting disorders, and chemotherapy agents used in cancer treatment. In addition, some cases develop without any identifiable cause — a pattern doctors call idiopathic avascular necrosis. Furthermore, conditions requiring long-term steroid use — including lupus and organ transplantation — carry particularly high osteonecrosis risk because disease-related vascular inflammation and immunosuppression both contribute independently.
Symptoms of Avascular Necrosis
The Silent Early Phase
Avascular necrosis bone tissue dies blood supply progresses silently in its earliest stages. Many people have no pain whatsoever when the condition first develops. This absence of symptoms during active bone death is one of the most clinically dangerous features of avascular necrosis — because by the time pain appears, significant bone damage has often already occurred.
Consequently, people with known risk factors — particularly those taking long-term corticosteroids, with sickle cell disease, or with a history of significant hip trauma — require proactive monitoring even in the absence of symptoms. Early-stage osteonecrosis shows no changes on standard X-ray. Therefore, MRI scanning is essential for detecting the condition before irreversible damage occurs.
Pain and Functional Decline
When symptoms do appear, pain in the affected joint is the most prominent feature. Hip osteonecrosis produces groin pain — sometimes radiating to the thigh or buttock — that initially occurs only during activity. As the condition progresses, pain appears at rest and during the night. The pain gradually becomes more severe and constant as bone collapse approaches.
Reduced range of movement in the affected joint develops alongside pain. People with hip osteonecrosis find it increasingly difficult to rotate the hip, walk distances, climb stairs, or put on shoes and socks. Moreover, a limp develops as the body unconsciously avoids loading the painful joint. In advanced disease — after joint surface collapse — the pain becomes severe and continuous, and joint function declines dramatically. Consequently, what began as mild groin discomfort can progress within one to two years to complete joint destruction if not diagnosed and treated promptly.
The symptom pattern of avascular necrosis overlaps significantly with osteoarthritis in its later stages. For a detailed comparison of joint pain conditions, see our article on osteoarthritis — inflammation, causes, and what actually helps.
How Doctors Diagnose Avascular Necrosis
Imaging Studies
Diagnosing avascular necrosis bone tissue dies blood supply requires imaging because clinical examination alone cannot confirm the diagnosis. Standard X-ray is the first investigation but detects osteonecrosis only in intermediate to advanced stages — when bone collapse or density changes become visible. In the critical early stage — when treatment has the most potential to save the joint — X-rays appear completely normal.
MRI scanning is the gold standard diagnostic tool for avascular necrosis. It detects bone marrow changes caused by osteonecrosis weeks to months before any changes appear on X-ray — providing a critical window for joint-preserving intervention. Furthermore, MRI accurately defines the size and location of the affected area, which directly influences treatment decisions and prognosis. Consequently, any patient with significant risk factors and hip or joint pain should undergo MRI rather than relying on normal X-ray findings to exclude the diagnosis.
CT scanning provides detailed three-dimensional imaging of bone structure and helps assess the degree of subchondral collapse — collapse of the bone just beneath the joint surface — in intermediate-stage disease. Bone scintigraphy — a nuclear medicine scan that detects increased bone turnover — was previously used for early diagnosis but has largely been replaced by MRI in most centres because of MRI’s superior sensitivity and specificity.
Blood Tests and Clinical Assessment
Blood tests do not directly diagnose osteonecrosis. However, they play an important role in identifying underlying causes. A full blood count and haemoglobin electrophoresis screen for sickle cell disease. Coagulation studies identify clotting disorders. Lipid profiles assess fat metabolism abnormalities. In addition, inflammatory markers and autoimmune antibodies help identify underlying conditions such as lupus or antiphospholipid syndrome that increase osteonecrosis risk.
Clinical assessment includes careful history-taking focused on steroid use duration and dose, alcohol consumption, prior joint trauma, and underlying medical conditions. Furthermore, a systematic review of all medications the patient takes helps identify drug-related causes. Consequently, combining thorough history-taking with MRI imaging gives the most complete picture of diagnosis, cause, and prognosis. For context on how kidney disease affects bone health and treatment complexity, see our article on chronic kidney disease — stages, symptoms, and how to slow the decline.
Treatment of Avascular Necrosis
Non-Surgical Treatment
Treatment of avascular necrosis bone tissue dies blood supply depends critically on the stage of the disease at diagnosis. Early-stage disease — before collapse of the joint surface — offers the most opportunity for joint-preserving treatment.
Reducing or eliminating the causative factor is the most important first step. Stopping or significantly reducing corticosteroid use, stopping alcohol, and treating underlying conditions such as sickle cell disease all reduce ongoing damage to bone vasculature. Furthermore, reducing weight-bearing on the affected joint — using crutches or a walking frame — lowers the mechanical stress on vulnerable bone tissue during the repair phase.
Medications including bisphosphonates — drugs that slow bone breakdown — and anticoagulants have been studied as potential treatments for early osteonecrosis. However, evidence for their effectiveness in preventing collapse remains limited and they are not standard first-line treatments. Vasodilators — drugs that widen blood vessels — and lipid-lowering agents are under investigation as potential protective therapies. Consequently, non-surgical management alone is most appropriate for very small lesions in low-risk locations rather than for large lesions threatening the weight-bearing joint surface.
Core Decompression
Core decompression is the most commonly performed joint-preserving surgical procedure for early-stage avascular necrosis. A surgeon drills one or more small tunnels through the outer bone into the area of osteonecrosis. This reduces the abnormally elevated pressure within the bone — improving blood flow to the affected area. Furthermore, the drilling stimulates the body’s own repair response by promoting new blood vessel growth into the decompressed zone.
Core decompression is most effective when performed before joint surface collapse occurs. It produces the best outcomes in small to medium lesions. Moreover, surgeons often combine it with bone grafting — filling the drill tunnel with bone graft material to provide structural support and further stimulate healing. Consequently, core decompression with bone grafting represents the best available joint-preserving option for appropriately selected early-stage patients.
Joint Replacement Surgery
For patients with advanced avascular necrosis — where the joint surface has already collapsed — joint replacement surgery is the most reliable and durable treatment. Total hip replacement removes the destroyed femoral head and acetabulum — the socket — and replaces them with metal, ceramic, and plastic components that recreate a smooth, pain-free joint surface.
Total hip replacement for avascular necrosis produces excellent pain relief and functional restoration in the majority of patients. However, patients with osteonecrosis tend to be younger than typical hip replacement patients. Consequently, implant longevity and the potential need for revision surgery later in life are important considerations in surgical planning and patient counselling.
For younger patients with collapse limited to a small area, more conservative surgical options — including osteotomy, which repositions the bone to shift loading away from the necrotic area — may preserve the natural joint for additional years before replacement becomes necessary. Furthermore, advances in surface replacement arthroplasty offer another option in carefully selected younger patients, preserving more of the original bone stock for potential future revision surgery.
Living Well After Avascular Necrosis Treatment
Rehabilitation and Recovery
Recovery from avascular necrosis treatment — whether core decompression or joint replacement — requires structured physiotherapy and rehabilitation. Progressive weight-bearing and strengthening exercises rebuild muscle around the repaired or replaced joint. Furthermore, cardiovascular conditioning supports overall recovery and reduces the deconditioning that accumulates during the period of reduced activity before and after surgery.
Return to normal activities typically occurs over three to six months after total hip replacement. Patients who have undergone core decompression require a longer protected weight-bearing period to allow healing before full loading resumes. Moreover, addressing the underlying cause — such as switching to steroid-sparing medications for autoimmune conditions or entering alcohol treatment programmes — reduces the risk of osteonecrosis developing in other joints after the initial affected joint is treated.
Monitoring for Bilateral and Multi-Joint Disease
Avascular necrosis frequently affects both hips simultaneously — even when symptoms are present in only one. Furthermore, in people with systemic risk factors such as high-dose steroid use or sickle cell disease, multiple joints can develop osteonecrosis concurrently or sequentially. Consequently, imaging of the opposite hip and other at-risk joints is recommended at diagnosis to detect asymptomatic disease before collapse occurs.
Regular follow-up with the treating orthopaedic surgeon monitors for disease progression, implant function after joint replacement, and new joint involvement over time. For context on managing chronic pain and joint conditions that can coexist with avascular necrosis, see our article on fibromyalgia — the pain condition that is real, widely misunderstood, and treatable.
When to Seek Urgent Medical Help
See a doctor promptly if you develop new groin, hip, or joint pain — particularly if you take corticosteroids, have a history of significant joint injury, or have a blood disorder such as sickle cell disease. Furthermore, any person with known risk factors who develops a sudden increase in joint pain or a noticeable change in gait needs urgent orthopaedic assessment without delay.
Consequently, do not assume groin or hip pain is simply muscular or age-related without proper investigation — early MRI scanning can identify avascular necrosis at a stage where joint-preserving treatment is still possible.
Frequently Asked Questions
1. How is avascular necrosis different from osteoarthritis?
Avascular necrosis results from bone cell death caused by loss of blood supply — typically producing rapid joint destruction over months to years. Osteoarthritis involves gradual cartilage breakdown and bone changes driven by mechanical and inflammatory factors over many years. Furthermore, avascular necrosis commonly affects younger people and progresses far more rapidly than osteoarthritis. Consequently, treatment decisions and urgency differ significantly between the two conditions despite producing similar symptoms in later stages.
2. Can avascular necrosis heal on its own?
In very small lesions — particularly in non-weight-bearing areas of bone — spontaneous healing occasionally occurs when the blood supply restores naturally and the necrotic area is small enough for the body’s own repair mechanisms to manage. However, large lesions — particularly those affecting the weight-bearing surface of the hip — rarely heal spontaneously. Consequently, proactive treatment rather than watchful waiting is recommended for most patients with confirmed avascular necrosis to prevent joint collapse.
3. Is steroid use always avoidable in conditions that cause avascular necrosis?
Not always. Many serious conditions — including lupus, severe asthma, and organ transplant rejection — require corticosteroids to manage life-threatening disease activity. In these situations, the benefits of steroid treatment outweigh the risk of osteonecrosis. Furthermore, using the lowest effective dose for the shortest necessary period, and switching to steroid-sparing agents when possible, reduces osteonecrosis risk significantly. Consequently, regular joint monitoring is appropriate for patients requiring prolonged high-dose steroid therapy.
4. Can both hips develop avascular necrosis at the same time?
Yes. Bilateral hip osteonecrosis — affecting both hips — occurs in roughly 40 to 80% of cases when the underlying cause is systemic — such as steroid use, sickle cell disease, or alcohol. Furthermore, one hip is often significantly more symptomatic than the other, leading patients and doctors to focus on the painful side while missing early asymptomatic disease in the opposite hip. Consequently, MRI of both hips is recommended at diagnosis when a systemic risk factor is present.
5. What is the long-term outlook after total hip replacement for avascular necrosis?
Total hip replacement produces excellent long-term outcomes for most patients with advanced avascular necrosis — significantly reducing pain and restoring joint function. Modern implants last 15 to 20 years in most patients. However, because avascular necrosis often affects younger patients than typical hip replacement candidates, revision surgery may be necessary during their lifetime. Consequently, choosing an experienced orthopaedic surgeon and following post-operative rehabilitation and monitoring recommendations closely gives the best possible long-term outcome.
Conclusion
Avascular necrosis is a serious and potentially devastating condition — silently destroying bone tissue from within until a joint collapses and function is lost. The loss of blood supply triggers a cascade that moves from invisible bone death to visible joint destruction with an urgency that demands early diagnosis and prompt action.
Avascular necrosis bone tissue dies blood supply affects people across all age groups, arises from several identifiable causes — many of which are modifiable — and responds best to treatment in its earliest stages. Furthermore, advances in MRI diagnostics, core decompression techniques, and joint replacement surgery mean that the outlook for people with this condition is significantly better today than it was even a decade ago.
If you have risk factors for avascular necrosis — including steroid use, heavy alcohol intake, sickle cell disease, or a significant joint injury — and develop new joint pain, speak to a doctor without delay. Consequently, early investigation and timely treatment give bone tissue and joint function the best possible chance of being preserved for years to come.
References
- Gaucher disease is classified into three types based on nervous system involvement and severity.
- Sickle cell disease is a genetic disorder affecting hemoglobin causing misshapen red blood cells, vaso-occlusive crises, hemolytic anemia, and multi-organ damage.
- You can feel hip pain at any stage of life, including childhood, young adulthood and the middle years.
Disclaimer
This article adapts publicly available information from WHO’s Musculoskeletal Conditions page. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform and not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.