
Kidney Cancer (Renal Cell Carcinoma): Symptoms, Types, and Treatment Options
When David went for a routine ultrasound to check for kidney stones—a problem that had plagued him periodically for years—his doctor found something unexpected: a 4-centimeter mass on his left kidney. David had no symptoms whatsoever. No pain, no blood in his urine, no weight loss. Just a chance finding during imaging for an unrelated issue. Biopsy confirmed renal cell carcinoma, stage I. “I felt completely fine,” David recalled. “If I hadn’t had that ultrasound, the tumor might have grown undetected for years.” David’s experience reflects a crucial reality about kidney cancer: it often produces no symptoms until advanced stages, and most cases today are discovered incidentally during imaging for other reasons.
Diagnosing patients with kidney cancer can be challenging. Renal cell carcinomas (RCCs), which make up the majority (85%) of kidney cancers, are characteristically insidious in onset. The once classical triad of haematuria, pain and abdominal mass is now recognised to be rare, and symptoms, if present at all, can be vague, non-specific and delayed in onset nih. While improved imaging has enabled earlier detection of asymptomatic tumors, understanding kidney cancer’s types, recognizing symptoms when they do appear, and knowing modern treatment options—particularly revolutionary immunotherapy advances—can make the difference between curable early-stage disease and advanced cancer requiring systemic therapy.
Understanding Kidney Cancer: What It Is And Who Gets It
The kidneys are two bean-shaped organs located behind the abdominal cavity on either side of the spine, just below the rib cage. Each kidney is about fist-sized and performs critical functions: filtering waste products from blood to produce urine, regulating blood pressure through hormone production, controlling red blood cell production through erythropoietin secretion, and maintaining electrolyte balance. Most people can live normally with one functioning kidney, which is why partial or complete kidney removal for cancer is feasible.
Renal cell carcinoma (RCC) is the most common type of kidney cancer. RCC forms in tiny tubes inside your kidneys called tubules. Tubules direct substances your body needs, like water and nutrients, to your bloodstream, while filtering waste through your urine (pee) Cleveland Clinic. RCC accounts for approximately 90% of kidney cancers in adults. The remaining 10% include transitional cell carcinoma of the renal pelvis (which behaves like bladder cancer), Wilms tumor (primarily affecting children), and rare sarcomas or other histologies.
Kidney cancer predominantly affects older adults. This review will focus mainly on renal cell carcinoma (RCC), which accounts for over 3% of all adult malignancies and has several histological subtypes. It is a tumor of older age group and is most commonly seen between the ages of 50 to 70 years that has an approximate 2:1 male to female ratio NCBI. Men develop kidney cancer roughly twice as often as women. Peak incidence occurs in the 60s and 70s, though kidney cancer can occur at any adult age. Racial differences exist, with Native Americans and Alaska Natives having highest incidence rates, followed by whites and blacks.
Risk factors for kidney cancer include smoking—the strongest modifiable risk factor—obesity (particularly in women), hypertension, chronic kidney disease, long-term dialysis, certain genetic conditions (Von Hippel-Lindau disease, hereditary papillary RCC, Birt-Hogg-Dubé syndrome), family history, and occupational exposures (asbestos, cadmium, certain organic solvents). The strongest risk factor for renal cell carcinoma (RCC) is smoking and not just cigarette smokers but also pipe, and cigar smokers are at higher risk. Obesity (especially in women) is another major risk factor. It is thought that the incidence of kidney cancers can be halved by eliminating tobacco smoking and excess body weight NCBI.
Types Of Renal Cell Carcinoma: Why Classification Matters
Not all kidney cancers behave the same way. Modern classification recognizes over 50 RCC subtypes based on cellular appearance, genetic alterations, and molecular profiles. Understanding your specific type matters because treatment responses and prognoses vary substantially. Clear cell renal cell carcinoma (ccRCC) is the most common type of RCC. There are more than 50 types of RCC in addition to ccRCC. Many are rare. Scientists classify them based on various factors, including how tumor cells look under a microscope and their DNA, or genetic material. Clear cell renal cell carcinoma (ccRCC): Up to 85% of RCCs are clear cell renal carcinoma. ccRCC gets its name from the way tumor cells look underneath a microscope — clear-colored. Papillary renal cell carcinoma: Ten percent to 15% of RCCs are papillary renal cell Cleveland Clinic.
Clear cell RCC represents 75-85% of all RCCs and generally carries intermediate prognosis. It’s characterized by cells appearing clear under microscope due to lipid and glycogen accumulation. Clear cell RCC arises from mutations in the VHL (von Hippel-Lindau) gene in most cases, which disrupts cellular response to oxygen levels and promotes blood vessel formation (angiogenesis). This biological characteristic makes clear cell RCC particularly responsive to anti-angiogenic targeted therapies and immunotherapy.
Papillary RCC comprises 10-15% of RCCs and subdivides into type 1 and type 2, with different genetic profiles and behaviors. Type 1 papillary RCC tends to have better prognosis, while type 2 can be more aggressive. Chromophobe RCC accounts for about 5% of cases and generally has favorable prognosis. Collecting duct carcinoma and medullary carcinoma are rare aggressive subtypes with poor outcomes. These distinctions matter clinically—clear cell RCC dominates clinical trial enrollment, so most treatment data applies primarily to this subtype.
Beyond histologic type, tumors are graded based on cellular appearance. Low-grade (grade 1-2) tumors have cells resembling normal kidney cells and grow slowly. High-grade (grade 3-4) tumors have very abnormal-appearing cells and behave aggressively. Tumor grade combines with stage to predict prognosis and guide treatment intensity. Molecular classification is increasingly important—certain genetic signatures predict treatment response, particularly to immunotherapy and targeted agents.
Symptoms: Often Silent Until Advanced
The sobering reality about kidney cancer is that most patients have no symptoms when small, curable tumors are present. While there are often no early signs of kidney cancer, some people may begin to experience symptoms once the tumor becomes larger and starts to affect nearby organs. Possible symptoms may include the following. Hematuria: Blood in the urine. This may be visible or detected only by urine testing. Fatigue: Extreme tiredness despite resting. Flank fullness: A feeling of pressure on one side of the lower back. Flank pain: Lower back pain on one side not caused by an injury City of Hope. The classic triad of hematuria (blood in urine), flank pain, and palpable abdominal mass—once considered diagnostic hallmarks—occurs in less than 10% of modern kidney cancer presentations and usually signals advanced disease.
Blood in urine represents the most common symptom when symptoms do occur. The blood may be visible (gross hematuria)—turning urine pink, red, or cola-colored—or microscopic (detected only on urinalysis). Unlike bladder cancer where hematuria is often the first sign prompting early diagnosis, kidney cancer hematuria tends to occur with larger tumors. The bleeding may be intermittent, appearing then disappearing for weeks or months. Any episode of gross hematuria warrants urological evaluation including imaging.
Flank or abdominal pain occurs in approximately 40% of symptomatic patients. The pain typically localizes to one side of the lower back or upper abdomen, dull and persistent rather than sharp. As tumors grow, they stretch the kidney capsule (the fibrous covering) causing discomfort. Very large tumors may create a palpable mass—something you or your doctor can feel as a firm lump in the abdomen or flank. By the time tumors are palpable, they’re usually quite large and advanced.
Systemic symptoms reflect advanced disease or paraneoplastic syndromes (effects from substances tumors produce). These include unexplained weight loss, persistent fatigue, recurrent fevers without infection, night sweats, loss of appetite, and anemia. Fatigue: Extreme tiredness despite resting. Weight loss: Weight loss within a short amount of time, without dieting. Loss of appetite: Not feeling hungry despite not eating. Anemia: Low red blood cell counts. Fever: A fever that keeps coming back even though there is no cold, flu or infection City of Hope. Some patients develop high blood pressure from tumor effects on kidney hormones. Men may develop varicocele—sudden swelling of scrotal veins—from tumor blocking the renal vein.
The challenge diagnostically is symptom nonspecificity. Fatigue, weight loss, and anemia occur with countless conditions. Flank pain suggests kidney stones or back problems. Even hematuria—the most specific symptom—more commonly results from UTIs, stones, or prostate disease. This is why many kidney cancers are discovered incidentally during CT scans or ultrasounds performed for other reasons—abdominal pain, trauma evaluation, or investigation of unrelated conditions.
Diagnosis: From Incidental Finding To Confirmation
The modern kidney cancer diagnostic pathway typically begins with imaging rather than symptoms. In the UK, incidence rates have risen by 47% over the past decade, with 12 000 new cases in 2015. By 2035, it is predicted that this number will rise to over 20 000 new cases per annum and kidney cancer will come to represent the fourth most common cancer among men and ninth most common among women in the UK nih. This rising incidence largely reflects increased use of abdominal imaging detecting incidental renal masses, not an epidemic of larger symptomatic cancers.
When kidney abnormalities are found, the workup proceeds systematically. CT scan with contrast (CT urography) is the gold standard for characterizing renal masses, determining size, location, enhancement pattern (how much contrast the mass absorbs), and relationship to kidney structures and surrounding organs. MRI provides similar information and is preferred when CT contrast is contraindicated (severe kidney dysfunction, contrast allergy). Ultrasound, while useful as an initial screening tool, cannot characterize masses as definitively as CT or MRI.
The critical imaging question is: cyst or tumor? Simple benign kidney cysts are extremely common—found in about 50% of people over 50—and require no treatment. These appear as round, fluid-filled structures with thin walls and no internal complexity on imaging. Complex cysts or solid masses require further evaluation. The Bosniak classification system categorizes renal cysts from I (simple, benign) to IV (clearly malignant), guiding management. Solid masses are presumed malignant until proven otherwise.
Unlike many cancers, kidney masses often don’t require biopsy before treatment. Imaging characteristics alone sufficiently distinguish malignant from benign masses in many cases, and surgical resection serves as both diagnosis and treatment. Renal mass biopsy is performed selectively: when imaging is indeterminate; when systemic therapy is considered without surgery (metastatic disease); to confirm metastatic disease from a suspected kidney primary; or when alternative diagnoses (lymphoma, abscess) are possible. Biopsy carries small risks—bleeding, infection, tumor seeding along needle tract—so it’s avoided when unnecessary.
Staging evaluation for diagnosed kidney cancer includes chest CT (lungs are the most common metastatic site), comprehensive metabolic panel (assessing kidney function and liver), and sometimes bone scan or brain imaging if symptoms suggest metastases. The TNM staging system classifies tumors by size and local extent (T), lymph node involvement (N), and distant metastases (M). This staging determines treatment approach and prognosis.
Survival And Prognosis: Stage Determines Outcome
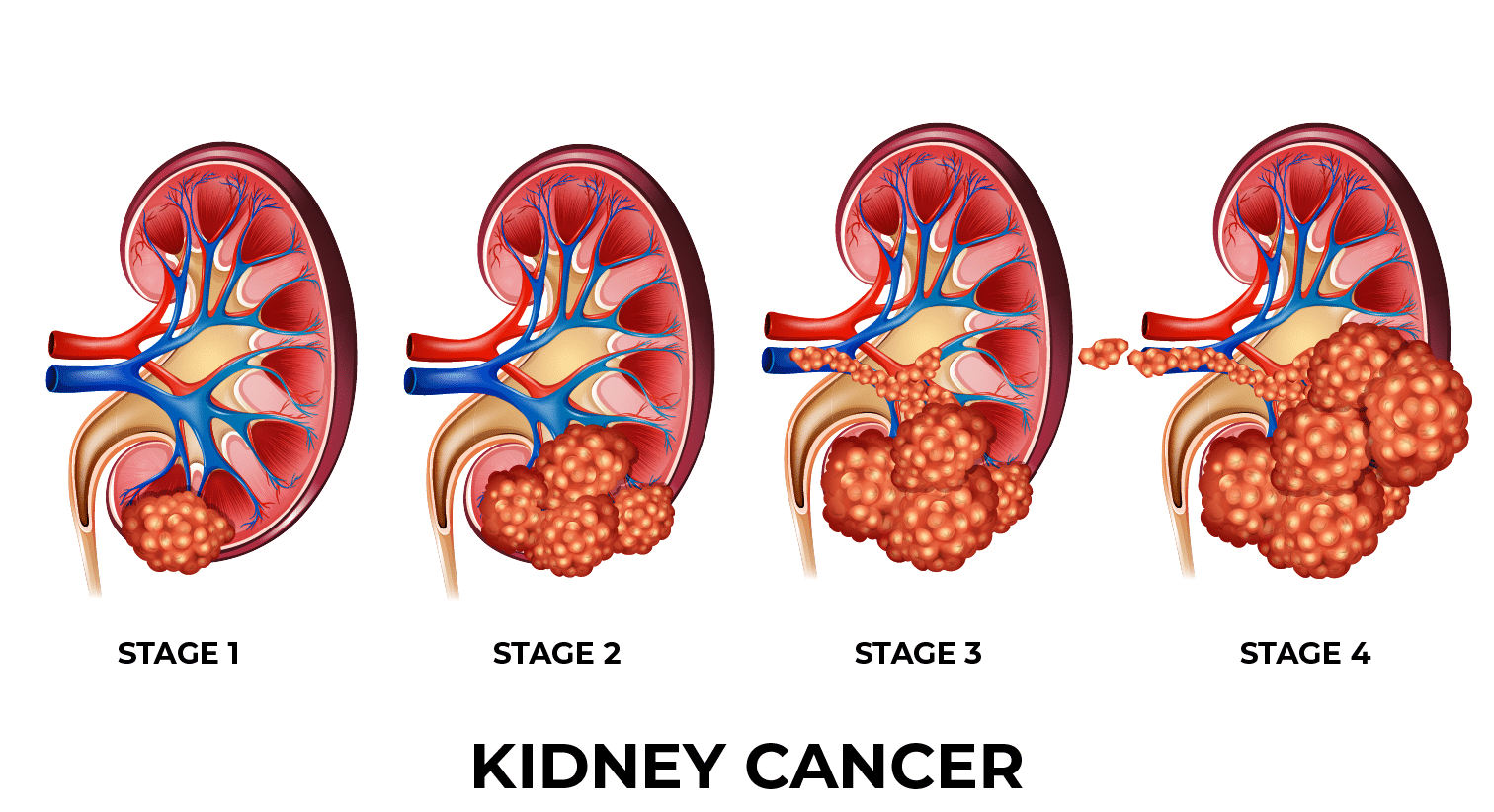
Kidney cancer prognosis varies dramatically by stage at diagnosis. For kidney and renal pelvis cancer, 65.7% are diagnosed at the local stage. The 5-year relative survival for localized kidney and renal pelvis cancer is 93.3% SEER Cancer Statistics. Localized disease—confined to the kidney without spread beyond the renal capsule—comprises about two-thirds of diagnoses and carries excellent prognosis. Five-year survival for stage I disease (tumor ≤7 cm confined to kidney) approaches 90-93%. Stage II (tumor >7 cm but still confined to kidney) has five-year survival around 75-80%.
Almost 90 out of 100 people (almost 90%) with stage 1 kidney cancer will survive their cancer for 5 years or more after they’re diagnosed. Around 75 out of 100 people (around 75%) with stage 2 kidney cancer will survive their cancer for 5 years or more after they’re diagnosed. Around 75 out of 100 people (around 75%) with stage 3 kidney cancer will survive their cancer for 5 years or more after they’re diagnosed. Around 15 out of 100 people (around 15%) with stage 4 kidney cancer will survive their cancer for 5 years or more after they’re diagnosed Cancer Research UK..
Stage III disease encompasses locally advanced cancer—tumor extending beyond kidney into major veins or adrenal gland, or involving regional lymph nodes. Five-year survival ranges from 50-75% depending on extent. Treatment typically involves surgery (when feasible) often combined with systemic therapy. Stage IV represents metastatic disease—cancer spread to distant lymph nodes, lungs, bones, liver, brain, or other organs. Five-year survival for metastatic disease historically was around 10-15%, though recent immunotherapy advances have substantially improved these numbers for some patients.
Beyond stage, other prognostic factors include: tumor grade (high-grade tumors behave more aggressively); histologic subtype (clear cell has different prognosis than papillary or chromophobe); presence of sarcomatoid or rhabdoid features (aggressive dedifferentiated components); performance status (how well patients function in daily activities); and laboratory values (anemia, elevated calcium, elevated inflammatory markers all predict worse outcomes). Prognostic models like the IMDC (International Metastatic RCC Database Consortium) score stratify patients into favorable, intermediate, and poor risk categories using these factors, guiding treatment selection.
Age and overall health significantly impact outcomes. Younger healthier patients tolerate aggressive treatments better and generally have superior survival independent of cancer characteristics. Comorbidities—heart disease, diabetes, chronic lung disease—limit treatment options and worsen prognosis. Kidney function before and after treatment affects systemic therapy tolerability and long-term quality of life.
Treatment For Localized Disease: Surgery Remains Gold Standard
For localized kidney cancer, surgery offers the highest cure potential. Standard treatment options include surgery (partial or radical nephrectomy, which is the removal of part or all of the kidney), targeted therapy, and immunotherapy. For newly diagnosed advanced or metastatic kidney cancer, immunotherapy is now a cornerstone of first-line treatment (the first treatment given for a disease) and has significantly improved survival outcomes over the past decade Cancer Research Institute. The surgical approach depends on tumor size, location, and patient factors.
Partial nephrectomy (nephron-sparing surgery) removes the tumor with a surrounding margin of normal kidney tissue while preserving the remainder of the kidney. This approach is standard for tumors under 4 cm (stage T1a) and increasingly used for tumors up to 7 cm when technically feasible. Partial nephrectomy offers equivalent cancer control to radical nephrectomy for appropriately selected tumors while preserving kidney function—an advantage that reduces long-term cardiovascular disease risk and chronic kidney disease progression.
Radical nephrectomy removes the entire kidney, surrounding fatty tissue, adrenal gland (sometimes), and regional lymph nodes (if enlarged or suspicious). This more extensive surgery is performed for large tumors, centrally located masses involving major vessels or collecting system, or multiple tumors within one kidney. Most patients tolerate radical nephrectomy well since the remaining kidney usually compensates, though some develop chronic kidney disease requiring monitoring.
Both surgeries can be performed through open incision, laparoscopically (minimally invasive through small incisions), or robotically-assisted (using robotic instruments controlled by surgeon). Minimally invasive approaches offer faster recovery, less pain, and shorter hospital stays with equivalent cancer outcomes for most tumors. Robotic surgery has particular advantages for complex partial nephrectomies requiring precise dissection and reconstruction.
For small renal masses in elderly or medically unfit patients, ablative therapies offer alternatives. Other minimally invasive techniques use either heat or cold to treat tumors in place, without having to remove any of the kidney. These are ideal for smaller kidney tumors in patients considered at high risk for surgery. Cryoablation freezes the tumor with a long, thin probe inserted into the tumor. Radiofrequency ablation (RFA) is similar to cryoablation, but heat is used to destroy the tumor instead of cold MD Anderson Cancer Center. These image-guided procedures destroy tumors without removing kidney tissue, though long-term cancer control data is less robust than surgery.
Active surveillance represents another option for small, slow-growing tumors in elderly or frail patients. Serial imaging monitors tumor growth; intervention occurs if growth accelerates or symptoms develop. About 20-30% of small renal masses are benign or very indolent cancers that may never cause problems, making surveillance reasonable in select cases.
Treatment For Advanced Disease: The Immunotherapy Revolution
The treatment landscape for metastatic kidney cancer has transformed over the past 15 years. Historically, metastatic RCC was largely resistant to traditional chemotherapy, with limited options offering modest survival benefits. Cytokine therapy (high-dose interleukin-2) worked for a small subset of patients but caused severe toxicity. Kidney cancer has a long history with immunotherapy. It was one of the first cancers to be treated with immune-based approaches. In 1992, high-dose interleukin-2 (IL-2) became the first immunotherapy ever approved by the U.S. Food and Drug Administration (FDA) for the treatment of any cancer, marking a pivotal milestone for the field Cancer Research Institute.
Targeted therapy arrived in the mid-2000s, revolutionizing kidney cancer treatment. These drugs target specific molecular pathways driving cancer growth. VEGF (vascular endothelial growth factor) inhibitors—sunitinib, pazopanib, axitinib, cabozantinib—block new blood vessel formation that tumors need for growth. mTOR inhibitors—temsirolimus, everolimus—interrupt cell growth signaling. These agents substantially improved progression-free and overall survival compared to prior treatments, establishing targeted therapy as the standard for years.
The next revolution came with immune checkpoint inhibitors. These antibodies release brakes on the immune system, enabling T-cells to recognize and attack cancer cells. Nivolumab (anti-PD-1) was the first checkpoint inhibitor approved for kidney cancer in 2015. Subsequently, combination approaches demonstrated superior results to single agents. Nivolumab plus ipilimumab (targeting PD-1 and CTLA-4 checkpoints) became a standard first-line option for intermediate and poor-risk metastatic clear cell RCC, offering unprecedented response rates and some patients achieving years of disease control.
Immunotherapy-targeted therapy combinations now dominate first-line treatment. Pembrolizumab (anti-PD-1) plus axitinib (VEGF inhibitor) showed improved survival over sunitinib alone. Avelumab (anti-PD-L1) plus axitinib demonstrated similar benefits. Nivolumab plus cabozantinib combined checkpoint blockade with multikinase inhibition, achieving high response rates. These combination regimens work synergistically—targeted therapy modulates the tumor microenvironment making it more susceptible to immune attack, while immunotherapy generates durable responses in some patients.
The impact extends beyond metastatic disease. For the first time in fifty years, results from a phase 3 randomized, placebo-controlled trial have shown an overall survival benefit from an adjuvant therapy in patients with kidney cancer. Treatment with pembrolizumab, an immunotherapy drug, after surgery significantly prolonged overall survival in patients with clear-cell renal-cell carcinoma (ccRCC) at high risk for recurrence. Pembrolizumab was associated with a 38% reduction in risk of death compared with placebo Dana-Farber Cancer Institute. The KEYNOTE-564 trial demonstrated that one year of adjuvant pembrolizumab after surgery for high-risk localized disease reduces recurrence and improves survival—the first adjuvant therapy to show overall survival benefit in kidney cancer.
Selection of systemic therapy considers multiple factors: disease risk stratification (IMDC score), prior treatments, comorbidities, patient preferences regarding side effect profiles, and molecular/histologic features. Some patients with favorable-risk disease may start with VEGF inhibitor monotherapy. Most intermediate and poor-risk patients receive combination immunotherapy or immunotherapy-targeted therapy combinations. Treatment continues until disease progression, unacceptable toxicity, or achievement of complete response in select cases.
Side Effects And Quality Of Life Considerations
Modern kidney cancer treatments—while more effective than historical options—carry significant side effects requiring management. Surgical complications include bleeding, infection, kidney function decline (particularly after radical nephrectomy), blood clots, and injury to surrounding structures. Minimally invasive approaches reduce some surgical risks but don’t eliminate them. Preserving kidney function through partial nephrectomy when possible improves long-term health.
Targeted therapy side effects vary by agent but commonly include fatigue, diarrhea, hand-foot syndrome (painful redness and peeling of palms and soles), hypertension, hypothyroidism, and mouth sores. VEGF inhibitors also cause proteinuria, bleeding tendency, and impaired wound healing. mTOR inhibitors cause mouth ulcers, metabolic abnormalities (elevated cholesterol and blood sugar), and pneumonitis (lung inflammation). Side effects are usually manageable with dose reductions, supportive medications, or treatment breaks, but significantly impact quality of life for many patients.
Immunotherapy toxicity differs from traditional chemotherapy—instead of predictable dose-related effects, checkpoint inhibitors cause immune-related adverse events where the activated immune system attacks normal tissues. Common manifestations include skin rash, diarrhea/colitis, thyroid dysfunction, liver inflammation, and fatigue. Less common but serious toxicities include pneumonitis, hypophysitis (pituitary inflammation), adrenal insufficiency, diabetes, myocarditis, and neurologic complications. Most immune toxicities are manageable with steroids and treatment interruption, but some require permanent discontinuation or chronic immunosuppression.
Combination regimens predictably cause more toxicity than single agents—the benefit of improved cancer control must be weighed against additive side effects. Treatment selection increasingly considers individual tolerance and priorities. An elderly patient valuing quality of life may prefer single-agent therapy with better tolerability over aggressive combinations. Younger patients seeking maximum cancer control may accept higher toxicity risk.
Supportive care interventions maintain quality of life during treatment: antiemetics for nausea, growth factors for anemia, skin care for hand-foot syndrome, thyroid replacement for hypothyroidism, antidiarrheals, pain management, nutritional support, and psychosocial services. Oncology teams including nurses, pharmacists, dietitians, social workers, and palliative care specialists provide comprehensive support beyond just cancer-directed therapy.
Surveillance And Follow-Up: Watching For Recurrence
Even after successful treatment for localized disease, kidney cancer can recur. Recurrence risk depends on original stage and grade—low-grade stage I tumors have under 5% recurrence risk, while high-grade stage III disease recurs in 30-50% of cases. Recurrences can occur in the remaining kidney, surgical bed, or distant sites (most commonly lungs). Most recurrences happen within the first 3-5 years, though late recurrences beyond 10 years occur more frequently with kidney cancer than many other malignancies.
Surveillance protocols use imaging to detect recurrences early when they remain potentially curable. Typical surveillance for partial nephrectomy or radical nephrectomy includes chest imaging (X-ray or CT), abdominal imaging (CT or MRI), and laboratory tests (kidney function, blood counts) at regular intervals—every 3-6 months initially, decreasing to annually after several years. Higher-risk tumors warrant more intensive surveillance. The goal is detecting small recurrences amenable to metastasectomy (surgical removal of isolated metastases) or early systemic therapy.
For patients with metastatic disease treated with systemic therapy, scans occur every 8-12 weeks to assess response. Treatment continues as long as disease remains controlled and side effects are tolerable. When disease progresses on one regimen, subsequent lines of therapy using different mechanisms are available—kidney cancer is increasingly managed as a chronic disease with sequential treatments over years.
Beyond cancer surveillance, kidney function monitoring is crucial for anyone who had nephrectomy. Remaining kidney function should be preserved through blood pressure control, diabetes management if present, avoiding nephrotoxic medications when possible, and maintaining adequate hydration. Cardiovascular risk reduction becomes important since chronic kidney disease increases heart disease risk.
Frequently Asked Questions
Q1: I have a small kidney mass found incidentally on CT. Does this mean I have cancer? Not necessarily. Many small renal masses are benign cysts requiring no treatment. Simple cysts are extremely common, found in about 50% of people over 50. However, solid masses or complex cysts warrant further evaluation since they’re more likely malignant. Your doctor will characterize the mass using imaging criteria (CT or MRI with contrast) and may recommend follow-up imaging, biopsy, or treatment depending on characteristics. Small solid masses have about 20-30% chance of being benign or very indolent tumors, but most require treatment or close surveillance since we can’t reliably distinguish aggressive from non-aggressive cancers without tissue sampling.
Q2: My kidney tumor is 3 cm. Do I need my whole kidney removed, or can they just remove the tumor? For a 3 cm tumor, partial nephrectomy (removing just the tumor while preserving the rest of the kidney) is likely the best option if technically feasible. Partial nephrectomy offers equivalent cancer control to radical nephrectomy for tumors under 7 cm when surgically achievable, with the major advantage of preserving kidney function. Preserving kidney function reduces long-term risks of chronic kidney disease, cardiovascular disease, and need for dialysis. Your urologist will assess tumor location—some centrally located tumors near major vessels are more challenging for partial nephrectomy. If partial nephrectomy isn’t feasible, radical nephrectomy (removing the whole kidney) is appropriate and most patients do well with one kidney.
Q3: I was diagnosed with stage IV kidney cancer. Does this mean I’m dying? Stage IV means cancer has spread beyond the kidney, which is serious and not curable by surgery alone. However, “stage IV” doesn’t mean imminent death or hopeless situation. Modern immunotherapy and targeted therapy combinations have dramatically improved outcomes for metastatic kidney cancer. Many patients live for years with good quality of life on treatment, and some achieve complete responses where all visible cancer disappears. While five-year survival for stage IV disease is around 15-20% overall, that statistic reflects older treatments—newer combination regimens are improving outcomes substantially. Survival varies widely based on extent of metastases, symptom burden, overall health, and treatment response. Focus on working with an experienced medical oncologist to develop a treatment plan maximizing both survival and quality of life.
Q4: I had my kidney removed for cancer five years ago and just had a lung nodule detected. Is this a recurrence? Possibly, yes. Lungs are the most common site of kidney cancer metastases, and recurrences can occur years after initial treatment. However, not all lung nodules in kidney cancer patients are metastases—they could be benign lesions, infections, or even new unrelated lung cancer. Your doctor will characterize the nodule with CT imaging and possibly PET scan. If imaging suggests metastasis, biopsy confirmation is often warranted before starting systemic therapy since treatment for kidney cancer metastasis differs from primary lung cancer. If confirmed as kidney cancer metastasis, solitary or few lung metastases may be surgically removable (metastasectomy), potentially offering cure or long-term control. Multiple or unresectable metastases require systemic therapy.
Q5: How often do small kidney tumors turn out to be benign? Should I consider just watching mine instead of surgery? Studies suggest 15-30% of small renal masses (under 4 cm) removed surgically are benign or very indolent cancers. This reality makes active surveillance (watching with serial imaging) reasonable for select patients—particularly elderly or frail patients who tolerate surgery poorly. However, we can’t reliably distinguish benign from malignant small masses without removing them, and some small tumors are aggressive cancers. Surveillance requires commitment to regular imaging and acceptance of some uncertainty. Most patients with reasonable surgical candidacy proceed with treatment (surgery or ablation) since cure rates approach 100% for small tumors when treated. Discuss your individual risk tolerance, surgical candidacy, tumor imaging characteristics, and surveillance compliance with your urologist to determine the best approach.
Disclaimer
This article adapts publicly available information from reputable medical sources and cancer research organizations. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform — not a healthcare provider. Decisions about kidney cancer screening, diagnosis, and treatment should be made in consultation with qualified urologists, medical oncologists, and other healthcare professionals who can evaluate your individual tumor characteristics, stage, overall health status, kidney function, and treatment goals. If you have been diagnosed with a renal mass or kidney cancer, please consult with your healthcare team promptly to discuss treatment options. Every patient’s situation is unique and requires personalized medical evaluation.
References
- Cleveland Clinic. Renal Cell Carcinoma: Symptoms, Treatment & Prognosis. https://my.clevelandclinic.org/health/diseases/24906-renal-cell-carcinoma
- PMC. Challenges of early renal cancer detection: symptom patterns and incidental diagnosis rate. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7223292/
- StatPearls. Renal Cancer. https://www.ncbi.nlm.nih.gov/books/NBK558975/
- Cancer Research Institute. Immunotherapy for Kidney Cancer. https://www.cancerresearch.org/immunotherapy-by-cancer-type/kidney-cancer
- Dana-Farber Cancer Institute. Immunotherapy post-surgery improves overall survival for kidney cancer. https://www.dana-farber.org/newsroom/news-releases/2024/immunotherapy-post-surgery-improves-overall-survival-for-kidney-cancer
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.