
Eosinophilic Esophagitis (EoE): The Food Allergy Condition Affecting the Food Pipe
There is a condition that was barely known to medicine three decades ago but is now being diagnosed with increasing frequency across the world, particularly in children and young adults. It causes difficulty swallowing, food getting stuck in the throat, chest pain, and in children, a refusal to eat that is often mistaken for behavioural problems or fussy eating. It is triggered by food allergens and environmental factors, driven by an overactive immune response, and for years it was routinely misdiagnosed as acid reflux — a condition it closely resembles but is fundamentally different from. That condition is Eosinophilic Esophagitis, almost always referred to by its abbreviation EoE.
Eosinophilic Esophagitis is a chronic, immune-mediated disease of the esophagus — the food pipe connecting the mouth to the stomach — in which a type of white blood cell called an eosinophil accumulates in abnormally large numbers in the esophageal lining. Eosinophils are part of the immune system and are normally found in small quantities in various tissues throughout the body. However, they are not normally present in the esophagus in significant numbers. When they accumulate there in response to allergen exposure, they release toxic proteins and inflammatory chemicals that damage the esophageal tissue, cause painful inflammation, and over time lead to scarring and narrowing of the food pipe that makes swallowing increasingly difficult and dangerous.
According to research published in major gastroenterology journals, EoE affects an estimated 1 in 2,000 people in Western countries, with prevalence rising steadily over the past three decades. The condition is approximately three times more common in males than females and is strongly associated with other allergic conditions — around 70% to 80% of EoE patients have co-existing allergic diseases including asthma, eczema, allergic rhinitis, or food allergies. The reasons for the rising incidence are not fully understood but are thought to involve changes in the microbiome, reduced early-life microbial exposure related to improved hygiene, increasing rates of food sensitisation, and possibly environmental allergen exposure.
Understanding the Immune Mechanism Behind EoE
To understand EoE properly, it helps to understand what eosinophils are and what happens when they appear where they should not be. Eosinophils are white blood cells that play a normal and important role in fighting parasitic infections and participating in allergic responses. In healthy individuals, the esophagus contains virtually no eosinophils — unlike the stomach and intestines, where small numbers are normal. In EoE, the immune system mounts an inappropriate allergic response to food antigens or, in some cases, airborne allergens, directing eosinophils to flood into the esophageal tissue.
Once these eosinophils accumulate in the esophagus, they become activated and release a range of inflammatory mediators — toxic granule proteins, cytokines, and other chemicals — that damage the surrounding tissue. This inflammation causes the esophageal lining to become swollen, rigid, and fragile. With repeated cycles of inflammation and healing, the body lays down scar tissue, causing the esophagus to gradually lose its normal flexibility and develop fibrous rings, furrows, and strictures — permanent narrowings that make it physically difficult for food to pass through. This combination of active inflammation and long-term structural remodelling is what distinguishes EoE from a simple allergic reaction and makes it a serious chronic disease requiring sustained management rather than occasional treatment.
Research has identified specific food antigens as the primary triggers for EoE. The most commonly implicated foods, identified through elimination diet studies, are milk, wheat, eggs, soy, nuts, and seafood — the so-called six-food elimination diet targets these categories specifically. Aeroallergens — pollen and other airborne allergens — are also thought to play a role in a subset of patients, which may explain why some EoE patients experience seasonal worsening of symptoms during high-pollen periods.
Symptoms Across Different Age Groups
One of the important features of EoE is that its symptoms differ meaningfully between children and adults, which has contributed to diagnostic delays and misdiagnosis across both age groups. In infants and toddlers, EoE typically presents as feeding difficulties, refusal to eat, failure to thrive, and vomiting. Because these are also common features of infant GERD and other feeding problems, EoE in very young children is frequently missed or treated as acid reflux for months or years before the correct diagnosis is made.
In school-aged children, abdominal pain, vomiting, and poor weight gain are the most prominent features. Children may avoid certain food textures — particularly meats, breads, and other foods that feel difficult to swallow — without being able to articulate exactly why. This avoidance behaviour is sometimes attributed to anxiety or sensory processing issues rather than a physical esophageal problem. In adolescents and adults, the symptom profile shifts toward the esophageal dysfunction that becomes increasingly dominant as scar tissue accumulates. Dysphagia — difficulty swallowing solid food — is the cardinal symptom in adult EoE and is present in the vast majority of diagnosed adults. Many adult patients describe developing elaborate behavioural adaptations to manage their swallowing difficulties: chewing food excessively, eating very slowly, cutting food into tiny pieces, drinking large amounts of liquid with meals to wash food down, or simply avoiding the foods that cause the most difficulty.
The most dramatic and alarming presentation of EoE is food impaction — a situation in which a piece of food, typically meat or bread, becomes lodged in the esophagus and cannot be swallowed or coughed back up. Food impaction is a medical emergency that requires endoscopic removal and is the presenting event that leads to EoE diagnosis in approximately 30% to 50% of adult patients. Chest pain, which can be severe and is sometimes mistaken for cardiac pain, is another common symptom, caused by the inflamed and spasming esophagus reacting to swallowing.
Why EoE Is So Often Misdiagnosed
The misdiagnosis of EoE as gastroesophageal reflux disease is one of the most documented problems in esophageal medicine. The two conditions share overlapping symptoms — heartburn, chest pain, regurgitation, and swallowing difficulties — and EoE was only formally characterised as a distinct disease in the early 1990s, meaning that for a long time it was not widely known or considered in differential diagnosis. Many patients with EoE are prescribed proton pump inhibitors for presumed GERD, experience partial or no improvement, and continue on an ineffective treatment path for years.
The distinction matters enormously because the underlying mechanisms and treatments are entirely different. GERD is caused by acid refluxing from the stomach into the esophagus due to a weakened sphincter. EoE is an immune-allergic condition in which eosinophils infiltrate the esophageal tissue in response to allergen exposure. Acid suppression alone does not address the allergic inflammation driving EoE. There is, however, an additional layer of complexity: a condition called PPI-responsive esophageal eosinophilia exists, in which some patients who meet the diagnostic criteria for EoE respond to proton pump inhibitor therapy — this overlap has made diagnosis and classification more nuanced in recent years and has led to ongoing revision of clinical definitions.
Other conditions that EoE is sometimes confused with include achalasia — a condition involving the failure of the esophagus to relax properly — esophageal strictures from other causes, and functional dysphagia. The definitive diagnosis of EoE can only be made through endoscopy with biopsy.
Diagnosis: Why Endoscopy and Biopsy Are Essential
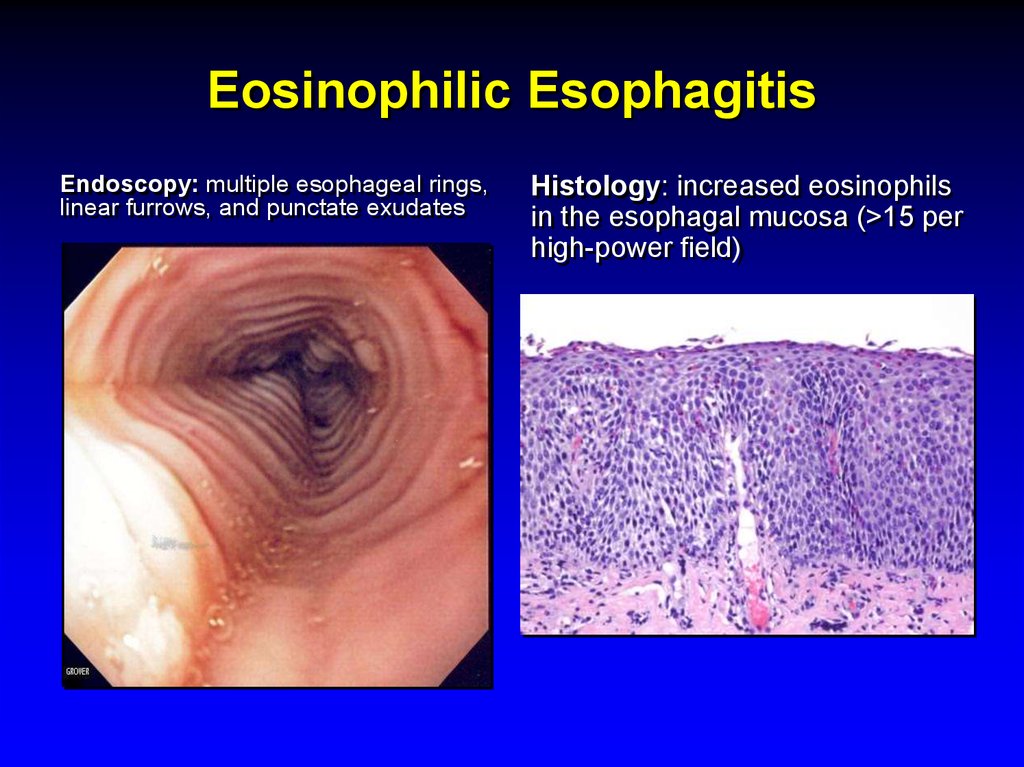
EoE cannot be diagnosed from symptoms or blood tests alone. The definitive diagnosis requires upper endoscopy, during which a gastroenterologist examines the esophageal lining and takes multiple biopsy samples from different levels of the esophagus. Under the microscope, a pathologist counts the number of eosinophils per high-power field — the current diagnostic threshold for EoE is 15 or more eosinophils per high-power field on biopsy, in the absence of other causes that might explain eosinophil accumulation.
During endoscopy, the gastroenterologist looks for characteristic visual features of EoE that are highly suggestive of the diagnosis even before biopsy results are available. These include concentric rings across the esophagus — giving it a corrugated or trachea-like appearance — longitudinal furrows or grooves running the length of the esophagus, white exudates or plaques on the esophageal surface, and narrowing of the esophageal lumen. A normal-appearing esophagus does not exclude EoE, however, as some patients have significant eosinophilic infiltration without visible endoscopic abnormalities, which is why biopsy is mandatory regardless of the endoscopic appearance.
Allergy testing — including skin prick tests and food-specific IgE blood tests — can help identify potential trigger allergens, though their predictive value for EoE specifically is limited compared to their usefulness in immediate-type allergic reactions. Patch testing and elimination diet trials are more commonly used to identify food triggers in clinical practice.
Treatment Approaches: Diet, Medication, and Dilation
The treatment of EoE is built around three main pillars: dietary therapy to remove allergenic triggers, pharmacological therapy to reduce eosinophilic inflammation, and endoscopic dilation to address strictures and narrowings that have already developed. In most cases, a combination of approaches is used, and treatment needs to be maintained long-term because EoE is a chronic condition with a high relapse rate when therapy is withdrawn.
Dietary therapy is particularly effective and is often the preferred first-line approach in children, who tend to tolerate elimination diets better than adults. The empiric six-food elimination diet — removing milk, wheat, eggs, soy, nuts, and seafood simultaneously — achieves histological remission in approximately 70% of patients and then allows systematic food reintroduction to identify specific triggers. A simpler two-food or four-food elimination diet targeting the most common triggers is also used in clinical practice, with somewhat lower but still meaningful remission rates. The challenge with dietary therapy is that it requires strict compliance, careful nutritional monitoring, and a lengthy reintroduction process that can take many months.
Pharmacological treatment primarily involves topical corticosteroids — fluticasone or budesonide — which are swallowed rather than inhaled, allowing the medication to coat the esophageal lining and reduce eosinophilic inflammation locally without the significant systemic side effects of oral steroids. Swallowed topical steroids achieve histological remission in approximately 50% to 70% of patients and are widely used as both induction and maintenance therapy. In 2022, the US Food and Drug Administration approved budesonide oral suspension specifically for EoE — the first medication formally approved for the condition — representing an important milestone in its recognition and management. Proton pump inhibitors continue to play a supporting role in some patients due to their anti-inflammatory properties in the esophageal mucosa.
For patients who have developed significant esophageal strictures or narrowings from chronic inflammation and scarring, endoscopic dilation — in which the narrowed esophagus is gently stretched using balloons or dilating instruments — provides mechanical relief of swallowing difficulties. Dilation does not treat the underlying eosinophilic inflammation and does not prevent further scarring, so it is used alongside anti-inflammatory therapy rather than as a substitute for it. For more health explainers like this one, visit ObserverVoice.com.
Frequently Asked Questions About Eosinophilic Esophagitis
1. Is EoE the same as a food allergy?
EoE is an allergic condition but it is not the same as a classic immediate food allergy. A classic food allergy — such as a peanut allergy — involves a rapid immune response mediated by IgE antibodies, causing symptoms within minutes of exposure including hives, swelling, and anaphylaxis. EoE involves a slower, chronic immune response primarily mediated by eosinophils and Th2 immune pathways, causing progressive inflammation in the esophagus rather than immediate systemic reactions. Many EoE patients have both types of allergic responses coexisting, but they are distinct mechanisms requiring different management approaches.
2. Can EoE be cured permanently?
Currently, EoE is considered a chronic condition without a definitive cure. Most patients require long-term dietary restrictions, ongoing medication, or both to maintain remission. When treatment is withdrawn, the majority of patients relapse within months. However, ongoing research into biologics — targeted immune therapies — is showing promising results. Dupilumab, a biologic medication that blocks key inflammatory pathways involved in EoE, received FDA approval for EoE in 2022 and represents a significant advance in treatment options for patients with moderate to severe disease.
3. How is EoE different from GERD?
GERD is caused by stomach acid refluxing into the esophagus due to a weakened lower esophageal sphincter, and it is treated with acid-suppressing medications. EoE is an immune-allergic condition in which eosinophils infiltrate the esophageal lining in response to food or environmental allergens, and it is treated with dietary elimination and topical corticosteroids. The two conditions share some overlapping symptoms but have completely different causes, mechanisms, and treatments. EoE does not respond reliably to acid suppression alone.
4. Can adults develop EoE or is it only a childhood condition?
EoE affects both children and adults and is increasingly diagnosed across all age groups. In children, feeding difficulties and vomiting are the most prominent features. In adults, dysphagia and food impaction are the dominant presentations. The rising incidence of EoE is being observed across all age groups, and adults who present with unexplained difficulty swallowing or recurrent food impaction should specifically be evaluated for EoE through endoscopy and biopsy.
5. Does EoE increase the risk of esophageal cancer?
Current evidence does not suggest that EoE significantly increases the risk of esophageal cancer. Unlike Barrett’s Esophagus — which is a recognised precancerous condition — EoE has not been convincingly associated with malignant transformation in clinical studies. The primary long-term risks of untreated EoE are progressive esophageal scarring, stricture formation, and increasing swallowing difficulty rather than cancer. This makes early diagnosis and sustained anti-inflammatory treatment important for preserving long-term esophageal function and quality of life.
References
- So, how can you avoid allergy symptoms?
- Allergy tests help doctors find out which foods might be causing your allergic reactions
This article adapts publicly available information from WHO’s digestive health resources and peer-reviewed medical literature. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform — not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.