
Mesenteric Ischemia: The Gut’s Version of a Heart Attack Explained
When the blood supply to your heart is suddenly cut off, the result is a heart attack. The heart muscle starves of oxygen, cells begin to die, and every minute without treatment increases the permanent damage. The same devastating process can happen to your gut.
Mesenteric ischemia is a serious condition in which the blood supply to the intestines becomes critically reduced or completely blocked. As a result, bowel tissue starves of oxygen, cells die rapidly, and — without immediate treatment — sections of the intestine can become gangrenous and life-threatening. Doctors often call it the gut’s version of a heart attack for precisely this reason.
Mesenteric ischemia gut heart attack comparisons are not merely metaphorical. The underlying mechanisms, the urgency of treatment, and the devastating consequences of delay are strikingly similar in both conditions. Furthermore, understanding this condition clearly can mean the difference between early diagnosis and a catastrophic outcome.
Quick Answer: What Is Mesenteric Ischemia?
Mesenteric ischemia is a condition in which the blood supply to part or all of the small intestine and large intestine becomes dangerously reduced. The mesenteric arteries and veins — the blood vessels supplying the bowel — become blocked, narrowed, or functionally inadequate. Consequently, bowel tissue is deprived of the oxygen and nutrients it needs to survive.
The condition exists in two main forms. Acute mesenteric ischemia develops suddenly and constitutes a surgical emergency. Chronic mesenteric ischemia develops gradually over time, causing recurring symptoms after eating. Moreover, both forms share the same fundamental problem — insufficient blood reaching the gut — but differ dramatically in their speed, severity, and treatment approach.
Why Doctors Call It the Gut’s Version of a Heart Attack
The heart attack comparison captures something essential about mesenteric ischemia gut heart attack parallels. In a heart attack, a blocked coronary artery cuts off blood to heart muscle. In acute mesenteric ischemia, a blocked mesenteric artery cuts off blood to bowel tissue. Both organs are highly metabolically active. Both sustain irreversible damage within hours of losing their blood supply. Furthermore, both conditions demand immediate intervention to prevent death.
The comparison extends to risk factors as well. Atherosclerosis — the buildup of fatty plaques inside artery walls — is the underlying driver of both conditions in many patients. The same risk factors that predispose a person to heart attack — advanced age, smoking, diabetes, hypertension, high cholesterol, and atrial fibrillation — also predispose them to mesenteric ischemia. Consequently, mesenteric ischemia and heart disease frequently coexist in the same patients.
However, the gut’s version of a heart attack carries an even higher mortality rate than cardiac ischemia. Acute mesenteric ischemia carries an overall mortality rate of 60 to 80% in many reported series, largely because diagnosis is frequently delayed. Therefore, recognising the warning signs early and acting with the same urgency applied to chest pain is absolutely critical.
The Blood Supply to the Gut
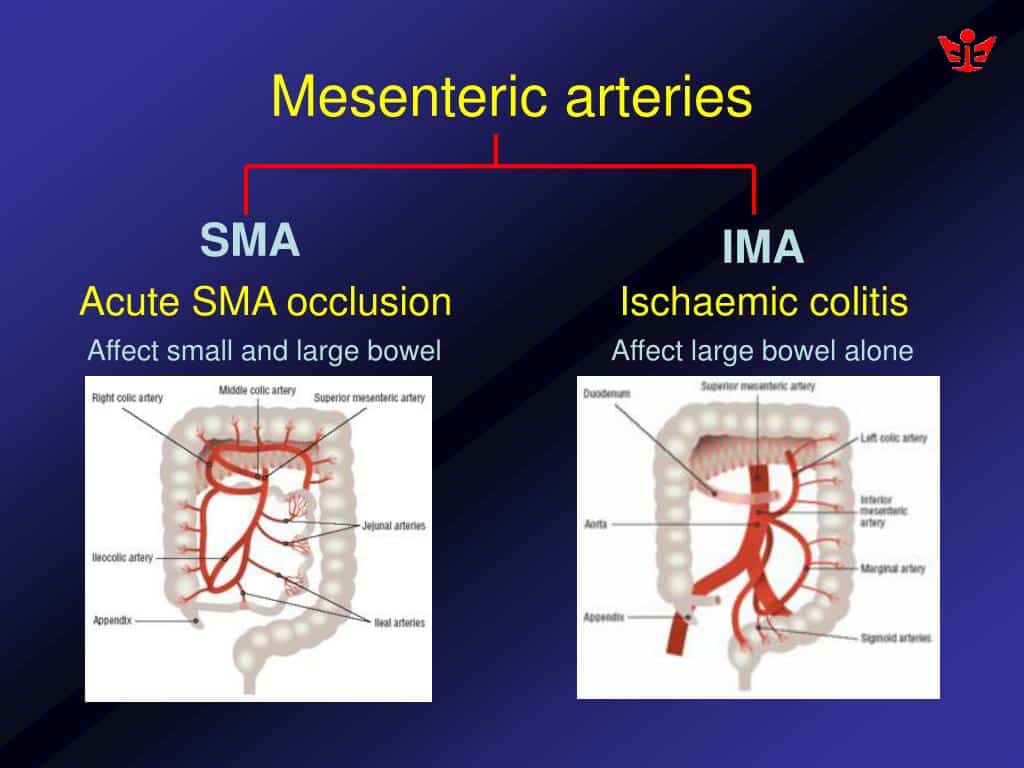
Understanding mesenteric ischemia requires a basic picture of how the bowel receives its blood supply. Three major vessels supply the intestines. The coeliac artery supplies the stomach, liver, and upper small bowel. The superior mesenteric artery — commonly called the SMA — supplies the entire small intestine and the right half of the large bowel. The inferior mesenteric artery — the IMA — supplies the left colon and rectum.
Of these three vessels, the superior mesenteric artery is the most critical and most commonly involved in mesenteric ischemia. It carries the largest volume of blood to the gut and has limited collateral circulation to compensate when it becomes blocked. Consequently, an acute occlusion of the SMA produces devastating ischemia across the majority of the small bowel in a matter of hours.
The mesenteric veins mirror this arterial supply. The superior mesenteric vein drains blood from the small bowel and right colon back toward the portal vein and liver. When venous drainage becomes obstructed, moreover, congestion builds inside the bowel wall and venous ischemia develops — a distinct and important subtype of mesenteric ischemia.
Types of Mesenteric Ischemia
Acute Mesenteric Ischemia
Acute mesenteric ischemia is the most dangerous form and demands the most urgent response. It develops rapidly, often within hours, and quickly progresses from reversible bowel ischemia to irreversible infarction — bowel death — without treatment.
Acute mesenteric ischemia has four distinct subtypes based on the underlying mechanism. Each requires a different treatment approach. Furthermore, correctly identifying the subtype guides the speed and nature of intervention.
Chronic Mesenteric Ischemia
Chronic mesenteric ischemia develops gradually as atherosclerotic plaques progressively narrow the mesenteric arteries over months or years. Blood flow at rest may remain adequate. However, after eating — when the bowel demands a significant increase in blood supply to digest a meal — the narrowed arteries cannot meet that demand. Consequently, the gut becomes temporarily ischemic after every meal, causing a characteristic pattern of postprandial pain.
This pattern leads to a phenomenon called food fear — patients deliberately avoid eating because they know a meal will trigger pain. As a result, significant unintentional weight loss is a hallmark feature of chronic mesenteric ischemia. Without treatment, moreover, chronic mesenteric ischemia can progress suddenly to acute occlusion and bowel infarction.
What Causes Mesenteric Ischemia?
The causes of mesenteric ischemia gut heart attack patterns differ depending on the type of ischemia involved. Understanding each cause is therefore essential for correct diagnosis and targeted treatment.
Arterial Embolism
Arterial embolism is the most common cause of acute mesenteric ischemia, accounting for approximately 40 to 50% of cases. A blood clot or other material breaks free from elsewhere in the body and travels through the bloodstream until it lodges in the superior mesenteric artery. In the majority of cases, the embolus originates from the heart — typically from a thrombus forming in the left atrium in patients with atrial fibrillation, or from a clot forming on a damaged heart valve or following myocardial infarction.
The embolus typically lodges just beyond the origin of the SMA, blocking blood flow to the majority of the small bowel almost instantaneously. Consequently, this subtype produces the most dramatic and rapidly progressive symptoms. Furthermore, the sudden nature of the occlusion gives collateral circulation no time to develop, which makes the ischemia particularly severe.
Arterial Thrombosis
Arterial thrombosis accounts for approximately 25 to 30% of acute mesenteric ischemia cases. In this subtype, a blood clot forms directly within the mesenteric artery at the site of a pre-existing atherosclerotic plaque. The plaque narrows the artery over years, and thrombosis occurs when the plaque ruptures or the flow dynamics change — in exactly the same way that coronary artery thrombosis causes a heart attack.
Because arterial thrombosis develops on a background of chronic atherosclerosis, many of these patients have pre-existing symptoms of chronic mesenteric ischemia before the acute event. Furthermore, they commonly have evidence of cardiovascular disease elsewhere — coronary artery disease, peripheral arterial disease, or prior stroke — reinforcing the systemic nature of atherosclerosis.
Mesenteric Venous Thrombosis
Mesenteric venous thrombosis accounts for approximately 5 to 15% of mesenteric ischemia cases. In this subtype, clotting occurs in the mesenteric veins rather than the arteries. As a result, venous outflow from the bowel becomes obstructed, blood congests within the bowel wall, and ischemia develops through a different mechanism — venous rather than arterial insufficiency.
Conditions predisposing to venous thrombosis include inherited clotting disorders such as factor V Leiden mutation and protein C or S deficiency, inflammatory bowel disease, intra-abdominal infection, portal hypertension, and malignancy. Additionally, oral contraceptive use and pregnancy elevate venous clotting risk. Mesenteric venous thrombosis tends to develop more slowly than arterial ischemia, which consequently gives a slightly wider diagnostic window.
Non-Occlusive Mesenteric Ischemia
Non-occlusive mesenteric ischemia, known as NOMI, accounts for approximately 20 to 30% of acute cases. In NOMI, no clot or physical obstruction blocks the mesenteric vessels. Instead, severe and sustained reduction in mesenteric blood flow occurs because of a profound physiological stress response. The mesenteric arteries constrict powerfully in response to shock, sepsis, heart failure, or major surgery, consequently reducing gut perfusion to critical levels despite the vessels remaining physically open.
NOMI is particularly associated with critically ill patients in intensive care settings. In addition, it carries a very high mortality rate because it is easily overlooked and frequently develops insidiously in patients who are already seriously ill from other causes. Moreover, the absence of a clear mechanical occlusion makes it diagnostically challenging.
Symptoms of Mesenteric Ischemia
Acute Mesenteric Ischemia Symptoms
Acute mesenteric ischemia presents with a characteristic clinical pattern that every clinician should recognise as a potential emergency. The classic presentation is sudden onset of severe periumbilical — around the navel — abdominal pain that is disproportionate to the physical findings on examination. This means the pain is excruciating, yet the abdomen may feel relatively soft and non-tender early in the course.
This disconnect between severe pain and apparently benign examination findings is a critically important clinical clue. Furthermore, it reflects the fact that in early ischemia the bowel wall is not yet infarcted and peritonitis has not yet developed. Consequently, clinicians who dismiss severe abdominal pain because the abdomen feels soft are at serious risk of missing this diagnosis.
Other early symptoms include nausea, vomiting, and urgent diarrhoea — sometimes bloody — as the ischemic bowel attempts to empty itself. As ischemia progresses to infarction, moreover, the abdomen becomes rigid and exquisitely tender, fever develops, and the patient deteriorates rapidly into septic shock.
Chronic Mesenteric Ischemia Symptoms
Chronic mesenteric ischemia produces a more subtle and gradual symptom pattern. Postprandial abdominal pain — pain occurring 15 to 60 minutes after eating and lasting one to three hours — is the defining symptom. The pain typically affects the central or upper abdomen and reflects the failure of narrowed arteries to supply the increased blood flow the gut needs after a meal.
Significant and progressive weight loss almost always accompanies the pain. Patients develop food fear — a conditioned avoidance of eating because of the predictable pain it causes. Furthermore, nausea, bloating, and altered bowel habits are common. In addition, an abdominal bruit — a whooshing sound heard through a stethoscope over the abdomen — may be present, reflecting turbulent blood flow through a narrowed mesenteric artery.
How Doctors Diagnose Mesenteric Ischemia
Clinical Suspicion and Blood Tests
Diagnosing mesenteric ischemia gut heart attack patterns requires a high degree of clinical suspicion. In acute cases, the combination of severe abdominal pain, relevant risk factors, and haemodynamic instability should immediately prompt investigation. Furthermore, any elderly patient with atrial fibrillation presenting with sudden severe abdominal pain must be assessed for mesenteric ischemia without delay.
Blood tests provide supporting but non-specific information in acute cases. Elevated lactate levels reflect anaerobic metabolism in ischemic tissue and are an important marker of severity. White cell count is typically elevated. In addition, elevated serum D-dimer, creatine kinase, and lactate dehydrogenase levels suggest tissue necrosis. However, normal blood tests do not exclude mesenteric ischemia, and consequently clinical suspicion must override reassuring laboratory results.
Imaging Studies
CT angiography of the abdomen and pelvis is the gold standard diagnostic investigation for mesenteric ischemia. It combines rapid availability, high sensitivity, and the ability to visualise the mesenteric vessels directly. Consequently, it can identify arterial occlusion, venous thrombosis, bowel wall ischaemia, and pneumatosis intestinalis — gas within the bowel wall signifying infarction — in a single study.
Conventional catheter angiography provides the most detailed imaging of mesenteric vessel anatomy. Furthermore, it carries the significant advantage of allowing immediate therapeutic intervention — such as thrombolysis or mechanical thrombectomy — in the same procedure. However, it is more invasive than CT and therefore reserved for cases where CT findings are inconclusive or immediate endovascular treatment is planned.
Duplex ultrasound can identify significant narrowing in the proximal mesenteric arteries and is useful for diagnosing chronic mesenteric ischemia in an outpatient setting. However, bowel gas frequently limits its accuracy in the acute setting. Moreover, it cannot assess the distal mesenteric vessels where emboli often lodge.
Treatment of Mesenteric Ischemia
Emergency Treatment of Acute Mesenteric Ischemia
Acute mesenteric ischemia constitutes a time-critical surgical emergency. Every hour of delay increases the extent of irreversible bowel infarction. Consequently, immediate resuscitation, anticoagulation, and urgent surgical or endovascular intervention must proceed simultaneously without waiting for all investigations to complete.
Intravenous fluid resuscitation restores circulating volume and supports blood pressure. Anticoagulation with heparin is initiated immediately to prevent clot propagation. Furthermore, broad-spectrum antibiotics address bacterial translocation from the ischemic gut. Vasopressor medications are avoided where possible because they further reduce mesenteric blood flow and consequently worsen ischemia.
Surgical and Endovascular Intervention
The choice between surgical and endovascular intervention depends on the subtype of ischemia, the clinical condition of the patient, and whether bowel infarction has already occurred. In patients without peritonitis, moreover, endovascular treatment — catheter-directed thrombolysis or mechanical thrombectomy — can restore blood flow without the need for open surgery.
Open surgical embolectomy or arterial bypass surgery is required when endovascular treatment fails, when peritonitis is present, or when bowel viability must be assessed directly. Furthermore, necrotic bowel requires surgical resection to remove dead tissue and prevent overwhelming sepsis. In some cases, a second-look laparotomy is performed 24 to 48 hours after initial surgery to reassess bowel viability once blood flow is restored.
Treatment of Chronic Mesenteric Ischemia
Chronic mesenteric ischemia requires revascularisation to restore adequate blood supply to the gut. Endovascular treatment — balloon angioplasty and stenting of the narrowed mesenteric artery — is now the preferred approach in most centres because it carries lower procedural risk than open surgery. Furthermore, it achieves excellent technical success rates and produces rapid symptom relief in the majority of patients.
Open surgical bypass is reserved for patients with complex anatomy not suitable for endovascular treatment, or for those in whom endovascular treatment has failed. Moreover, long-term antiplatelet therapy and aggressive management of cardiovascular risk factors — including statin therapy, blood pressure control, smoking cessation, and diabetes management — are essential components of post-revascularisation care.
Treatment of Mesenteric Venous Thrombosis and NOMI
Mesenteric venous thrombosis is primarily treated with anticoagulation. Most patients respond well to therapeutic anticoagulation with heparin followed by long-term oral anticoagulation. Furthermore, the underlying prothrombotic condition requires identification and treatment. Surgical intervention is reserved for patients with peritonitis or bowel infarction.
NOMI treatment focuses on correcting the underlying physiological cause — restoring cardiac output, treating sepsis, and reversing shock. In addition, intra-arterial papaverine — a vasodilator — can be infused directly into the superior mesenteric artery through an angiography catheter to reverse mesenteric vasoconstriction. Consequently, this approach is most effective when initiated early before infarction occurs.
Prevention of Mesenteric Ischemia
Prevention of mesenteric ischemia gut heart attack events is closely aligned with the prevention of cardiovascular disease more broadly. Therefore, managing the shared risk factors aggressively reduces the risk of both conditions simultaneously.
Anticoagulation therapy in patients with atrial fibrillation significantly reduces the risk of cardiogenic embolism to the mesenteric arteries. Consequently, appropriate anticoagulation in atrial fibrillation prevents a substantial proportion of embolic mesenteric ischemia cases. Furthermore, statin therapy slows the progression of atherosclerosis in the mesenteric arteries, reducing the risk of thrombotic occlusion over time.
Smoking cessation is one of the most powerful interventions available. Smoking accelerates atherosclerosis, promotes thrombosis, and causes mesenteric vasoconstriction — three mechanisms that all directly increase mesenteric ischemia risk. In addition, controlling blood pressure, managing diabetes effectively, and maintaining a healthy weight all reduce the atherosclerotic burden in the mesenteric circulation.
Living With Chronic Mesenteric Ischemia
Many people live with undiagnosed chronic mesenteric ischemia for months or years before the condition is recognised. After successful revascularisation, moreover, the transformation in quality of life is often dramatic. Postprandial pain resolves, food fear disappears, and patients are able to eat normally and regain lost weight.
Long-Term Monitoring After Treatment
Regular follow-up imaging is essential after revascularisation to detect restenosis — re-narrowing of the treated vessel — before symptoms recur. Duplex ultrasound surveillance every six to twelve months is therefore standard practice in most vascular surgery centres. Furthermore, recurrence of symptoms — particularly the return of postprandial pain or unexplained weight loss — should prompt urgent reassessment.
Long-term medication adherence is equally important. Antiplatelet therapy, statin therapy, and antihypertensive medications must continue indefinitely to protect both the mesenteric circulation and the broader cardiovascular system. Moreover, lifestyle modifications — healthy diet, regular exercise, smoking avoidance — support long-term vascular health and consequently reduce the risk of disease recurrence.
When to Seek Urgent Medical Help
Seek emergency medical care immediately if you experience sudden and severe abdominal pain — particularly if it seems out of proportion to what the abdomen feels like from the outside. Any combination of severe abdominal pain with nausea, vomiting, bloody diarrhoea, or rapid clinical deterioration warrants emergency evaluation without delay.
Furthermore, anyone with known atrial fibrillation, recent heart attack, or established cardiovascular disease who develops sudden severe abdominal pain should be assessed for mesenteric ischemia as a priority. Consequently, informing emergency medical staff about your cardiac history immediately helps ensure the correct investigations are requested without delay.
If you have previously experienced postprandial pain and unintentional weight loss, moreover, speak to your doctor about investigation for chronic mesenteric ischemia before an acute event occurs. Early diagnosis and elective revascularisation carry dramatically better outcomes than emergency treatment of acute bowel infarction.
Frequently Asked Questions About Mesenteric Ischemia Gut Heart Attack
1. Why is mesenteric ischemia so difficult to diagnose?
Mesenteric ischemia is difficult to diagnose because its early symptoms — abdominal pain, nausea, and vomiting — overlap with dozens of more common and less serious conditions. Furthermore, the classic finding of pain disproportionate to physical examination findings is subtle and easily missed. Consequently, diagnosis is frequently delayed, which explains the high mortality rate associated with the acute form.
2. What is the survival rate for acute mesenteric ischemia?
Survival rates vary considerably depending on how quickly diagnosis and treatment occur. When treatment begins before bowel infarction develops, survival rates are substantially higher. However, once infarction occurs, reported mortality rates range from 60 to 80% in many series. Consequently, every hour of diagnostic delay directly worsens the prognosis.
3. Can mesenteric ischemia be mistaken for other conditions?
Yes, frequently. Acute mesenteric ischemia is commonly mistaken for other causes of acute abdominal pain including pancreatitis, bowel obstruction, perforated ulcer, and renal colic. Furthermore, chronic mesenteric ischemia is often misdiagnosed as irritable bowel syndrome, peptic ulcer disease, or functional abdominal pain for months or years. Consequently, a high index of clinical suspicion is essential in patients with relevant risk factors.
4. Is mesenteric ischemia hereditary?
Mesenteric ischemia caused by atherosclerosis is not directly hereditary. However, the underlying risk factors — including familial hypercholesterolaemia, inherited hypertension, and inherited clotting disorders such as factor V Leiden mutation — can run in families. Therefore, a strong family history of cardiovascular disease or venous thrombosis warrants early risk factor assessment and management.
5. Can the bowel recover after mesenteric ischemia?
Recovery depends on the duration and severity of ischemia. Bowel that has been ischemic but not yet infarcted can recover function after blood flow is restored. However, infarcted bowel is irreversibly dead and must be surgically removed. In cases requiring extensive bowel resection, moreover, patients may develop short bowel syndrome — a condition in which insufficient bowel remains to absorb adequate nutrition. Consequently, nutritional support becomes a long-term necessity in these cases.
References
- Moyamoya disease is a rare progressive cerebrovascular disorder characterized by progressive stenosis of distal internal carotid arteries and abnormal collateral vessel development.
- Giant Cell Arteritis causes variable symptoms depending on which arteries are involved.
- The exact cause of arterial narrowing in moyamoya disease remains incompletely understood.
- Antiphospholipid syndrome is an autoimmune thrombotic disorder characterized by recurrent blood clots and/or pregnancy complications in the presence of antiphospholipid antibodies.
- Antiphospholipid Syndrome causes variable symptoms depending on whether thrombotic events have occurred and whether pregnancy is involved.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. It is not a substitute for professional diagnosis, treatment, or guidance from a licensed healthcare provider. If you have symptoms of mesenteric ischemia or any other medical condition, please consult a qualified doctor promptly. Always follow the advice of your healthcare team for your individual health needs.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.