
Wilms Tumor (Nephroblastoma): The Kidney Cancer Found in Children
Imagine a four-year-old boy whose parent notices abdominal swelling. Mild. Protruding. Attributed to normal childhood. Observation. Weeks pass. Swelling increases visibly. Parent concerned. Physician examination. Abdominal mass palpable. Firm. Fixed. Concerning. Imaging ordered urgently. Abdominal ultrasound. Large renal mass. Left kidney. Heterogeneous. Enhancement. Malignancy suspected. CT abdomen. Large mass. Left kidney. Intrarenal origin. Tumor extent determined. MRI renal. Mass characteristics detailed. Crossing midline. Risk vascular. Involvement. Staging evaluation. CT chest. Lungs. Metastases screening. Chest clear. Metastatic disease absent. Diagnosis obtained. Biopsy tissue. Wilms tumor. Favorable histology. Stage 2. Risk stratification favorable. Treatment planning. Chemotherapy neoadjuvant. Pre-operative planned. Chemotherapy cycles. Multiple. Months duration. Tumor response excellent. Significant shrinkage. Imaging shows. Surgery scheduled. Partial nephrectomy attempted. Technically challenging. Tumor large remaining. Complete nephrectomy performed. Left kidney removed. Specimen pathology. Favorable histology confirmed. Complete resection. Negative margins. Achieved. Chemotherapy continued. Post-operative. Additional cycles. Completion. Months total chemotherapy. Radiation abdomen. Not indicated. Favorable histology. Stage 2. Low-risk disease. Observation. Planned. Surveillance imaging. Regular. Months. Years. No recurrence. Five years. Cure achieved. He returns. Normal activities. School. Play. Sports eventually. Kidney function. Right kidney. Adequate. Normal life. Possible. Renal function preserved sufficiently. Dialysis unnecessary. Understanding Wilms tumor enables early recognition of this highly curable pediatric renal malignancy and appropriate treatment enabling survival and renal function preservation. Wilms tumor is a malignant embryonal kidney tumor arising from immature renal tissue characterized by pediatric predominance, genetic basis (WT1 gene), and excellent prognosis with modern treatment. Wilms tumor accounts for approximately 5 to 6 percent of childhood cancers. Approximately 400 to 500 new cases annually in the United States. Approximately 7,000 to 8,000 new cases annually worldwide. Peak incidence. Age 3 to 5 years. Approximately 90 percent diagnosed before age 8. Rare after age 10. Unilateral disease. Approximately 95 percent. Bilateral synchronous. Approximately 5 percent. What makes Wilms tumor important to understand is recognizing that while it is a serious malignancy, modern multimodal therapy enables cure in approximately 90 percent of children with many achieving preserved renal function enabling normal kidney function without dialysis. Early diagnosis through awareness of warning signs and appropriate staging is critical. Understanding Wilms tumor enables early recognition of this highly curable pediatric malignancy and appropriate treatment enabling survival and renal preservation. In this comprehensive article, we will explore what Wilms tumor is, understand the genetic basis and syndromic associations, recognize clinical presentations often initially misdiagnosed, explore diagnostic imaging and staging, and discover treatment outcomes and prognostic factors.
Understanding Renal Development and Wilms Tumor Pathophysiology
Before we explore Wilms tumor, we need to understand normal renal development and how malignant transformation occurs in immature renal cells. Kidney anatomy. Kidneys bilateral. Retroperitoneal. Positioned laterally. Vertebral column. Bean-shaped. Approximately 10 to 12 centimeters. Length. Approximately 5 to 7 centimeters. Width. Approximately 2 to 3 centimeters. Thickness. Blood supply. Renal artery. Branches. Lobar arteries. Segmental. Interlobar. Arcuate arteries. Interlobular. Flow hierarchic. Blood pressure regulation. Filtration. Glomerular. Renal function critical. Kidney internal structure. Three regions. Cortex. Outer. Glomeruli. Proximal. Distal. Tubule portions. Medulla. Inner. Loop Henle. Collecting ducts. Pelvis. Funnel. Ureter. Urine. Collection. Transport bladder. Nephrogenesis. Kidney development. Embryonic. Three successive. Systems mesonephros. Pronephros initial. Functional briefly. Weeks 3-4 gestation. Degenerates. Mesonephros. Weeks 5-8 gestation. Functional some. Fetal kidney filtration. Metanephros. Weeks 5-36 gestation. Definitive kidney. Ureteric bud. Ureter development. Branching. Collecting system. Formation. Collecting ducts. Calyces. Major minor. Ureteric bud. Mesenchymal tissue. Reciprocal induction. Interaction epithelial-mesenchymal. Metanephric mesenchyme. Metanephric blastema. Undifferentiated. Nephrogenic zone. Peripheral cortex. Fetal kidney. Nephrogenesis. Continues weeks 5 to 36. Gestation. Last glomeruli. Formation weeks 34-36. Postnatal maturation. Continuing. Filtration capacity. Increases. GFR. Glomerular filtration. Rate. Maturation progressive. Neonatal. Childhood. Nephrogenesis completion. Approximately 1 to 2 years. Postnatal. Glomerular number fixed. Birth. No new glomeruli. Formation postnatal. Pre-existing glomeruli. Maturation. Enlargement. Function. Improvement. Progressive. Kidney development control. Molecular signaling. Complex. WT1 gene. Wilms tumor suppressor. Transcription factor. Zinc finger protein. WT1. Critical. Mesodermal development. Gonadal. Urogenital structures. WT1. Expression. Fetal kidney. Stromal cells. Podocytes. Supporting. WT1. Essential. Urogenital development. Mutations. Developmental abnormalities. Associated. WAGR syndrome. WT1 deletion. Associated. Aniridia. Genitourinary abnormalities. Retardation mental. Syndrome complex. Denys-Drash syndrome. WT1 mutation. Mesangial sclerosis. Diffuse glomerulonephritis. Progressive renal failure. Pseudohermaphroditism. Males. Gonadal dysgenesis. Possible. Beckwith-Wiedemann syndrome. Bilateral Wilms. Risk. Elevated approximately 5 to 10 percent. Hemihypertrophy. Macroglossia. Omphalocele. Features characteristic. Tumor suppressor genes. Other. WT1. Primary. CTNNB1. Beta-catenin. Wnt signaling. Gene. Mutations approximately 15 to 20 percent. MYCN amplification. Possible. TP53 mutation. Approximately 5 to 10 percent. High-risk disease. Associated. Loss 16q. Approximately 5 to 10 percent. Unfavorable histology. Associated. Wilms tumor development. Mechanisms. WT1 inactivation. Loss biallelic. Required. Knudson two-hit hypothesis. Embryonal renal cells. WT1. Mutation germline or somatic. Second mutation somatic. Cell tumor. Malignant transformation. Additional genetic alterations. Cooperation required. Transformation acceleration. Cell of origin. Nephrogenic rest. Hypothesis. Abnormal nephrogenic tissue. Persisting. Infancy. Childhood. Risk. Malignant transformation. Perilobar nephrogenic rests. PLNR. Beckwith-Wiedemann syndrome. Associated. Intralobar nephrogenic rests. ILNR. Associated. Denys-Drash syndrome. Nephroblastomatosis. Bilateral. Multiple foci. Nephrogenic rests. High-risk. Bilateral Wilms. Development. The pathophysiology explains how WT1 loss and additional genetic alterations drive Wilms tumor development in immature nephrogenic tissue.
What is Wilms Tumor?
Wilms tumor is a malignant embryonal kidney tumor arising from immature metanephric mesenchyme characterized by pediatric predominance, genetic basis (WT1 gene), and excellent prognosis with modern therapy. Definition. Malignant renal. Embryonal kidney tumor. Children predominantly. Arises immature renal tissue. Metanephric blastema. Nephrogenic zone. Embryonal. Origin reflected. Histology. Triphasic. Blastematous. Epithelial. Stromal tissue. Components present. Variations. Degrees differentiation. Histologic classification. Favorable histology. Approximately 90 percent. Unfavorable histology. Approximately 10 percent. Anaplasia. Nuclear enlargement. Hyperchromasia. Abnormal mitoses. Unfavorable. Associated. Poor prognosis. Prognostic significance high. Histology. Stage. Biology combined. Risk determination. Bilateral Wilms. Synchronous. Same time. Metachronous. Sequential. One kidney then other. Time-delayed. Months years. Between. Bilateral disease. Approximately 5 to 10 percent all Wilms. Genetic predisposition. WT1 germline. Bilateral risk higher. Management. Both kidneys affected. Kidney preservation. Challenging. Chemotherapy often effective. Shrinkage tumor. Nephron-sparing. Surgery possible. Bilateral complete nephrectomy. Dialysis-dependent. Avoided. Preferred. Metastatic spread. Lungs approximately 80 to 85 percent common site. Liver approximately 10 percent. Bone marrow. Lymph nodes regional. Brain. Rare. Metastases present diagnosis approximately 10 to 15 percent. Prognostic implication. Staging. TNM classification. Tumor size. Node involvement. Metastases. Stage 1. Confined kidney. Completely resectable. No metastases. Stage 2. Extends beyond kidney. Resectable completely. No metastases. Stage 3. Not completely resectable locally. Lymph node involvement. Positive margins. Metastases. Local. Stage 4. Hematogenous. Lymphatic metastases. Distant organs. Stage 5. Bilateral synchronous. Kidney involvement. Both. Prognostic factors. Histology favorable or unfavorable. Stage 1-5. Age at diagnosis younger. Better. Genetics WT1 loss. Loss biallelic. Worse. MYCN amplification. Loss 16q. Unfavorable. Metastases present. Prognosis worse. Tumor size large prognosis. Relatively independent. But operative difficulty. Vascular involvement. Increases. Risk. Renal artery. Vein. Inferior vena cava. Involvement. Surgical challenge. Tumor thrombus. Vena cava. Extension. Surgical complexity. Increased. Prognosis. Overall Wilms. Modern. Approximately 90 percent. Five-year survival. Favorable histology. Stage 1. Approximately 98 to 99 percent. Unfavorable histology. Metastases. Approximately 40 to 50 percent. Intermediate outcomes. Appropriate therapy. Cure achievable. Majority cases. The clinical features reflect variable biological behavior from excellent-prognosis favorable histology localized to challenging unfavorable histology metastatic disease.
Recognizing Wilms Tumor: Clinical Presentations and Diagnostic Challenges
Wilms tumor has characteristic clinical presentations recognizable by abdominal mass and hematuria often initially misdiagnosed as urinary tract infection or benign condition. Abdominal mass presentation (most common). Young child age 3 to 6 years. Parent notices abdominal swelling. Enlargement visible. Progressive. Weeks. Months. Firmness. Palpable. Mass. Child usually asymptomatic. Healthy appearance. Normal activity levels. Mass finding. Incidental often. Parent physician examination. No pain. Usually. No systemic symptoms. Constitutional. Examination abdominal mass firm fixed. Tenderness minimal. Bilateral kidneys assessed. Unilateral versus bilateral. Determination. Imaging ordered ultrasound. Renal mass visualized. Hypoechoic heterogeneous. Enhancement. MRI ordered detailed anatomy. Mass size. Location. Vascular involvement. Assessed. CT chest lungs. Metastases screening. Metastases absent most cases. Stage 1 or 2. Favorable. Treatment planning initiated. Chemotherapy neoadjuvant. Pre-operative planned. Chemotherapy response assessed serial imaging months. Surgery delayed chemotherapy completion. Nephrectomy performed. Specimen pathology. Prognosis determined. Hematuria presentation (less common). Young child. Gross hematuria. Blood urine visible. Red-colored. Alarming appearance. Parent concerned. Pediatrician consultation. Urinary tract infection suspected. Urine culture obtained. Infection absent. Ultrasound ordered. Hematuria etiology investigation. Renal mass. Visualized. Wilms tumor. Considered. CT MRI. Staging imaging. Metastases screening. Performed. Treatment plan established. Hematuria. Associated malignancy. Common initially considered. But Wilms. Differential important. Renal colic kidney stone. Glomerulonephritis. IgA nephropathy. Other hematuria causes. Considered ruled. Imaging. Diagnostic clarity. Essential. Elevated blood pressure presentation. Young child. Hypertension. Elevated. Blood pressure screening. Incidental finding. Hypertension mechanism. Wilms tumor. Renin production. Increased. Possible. Renal artery compression. Tumor mass. Pressure effect. Possible. Hypertension. Secondary. Tumor mass. Related. Imaging. Renal mass. Wilms. Diagnosed. Blood pressure. Normalizes post-nephrectomy. Usually. Hypertension resolution. Post-operative. Expected. Constitutional symptoms presentation. Child. Fever. Weight loss. Failure thrive. Malaise. Nonspecific symptoms. Viral infection. Suspected initially. Illness atypical. Months duration. Persistent. Imaging indicated. Fever etiology investigation. Renal mass. Incidentally discovered. Wilms tumor. Diagnosed late presentation. Advanced stage possible. Constitutional symptoms. Associated. Tumor burden. Large. Systemic inflammation. Cytokine production. Fever generation. Possible mechanism. Anemia. Pallor. Fatigue. Associated. Blood loss. Hematuria chronic. Possible. Bone marrow involvement. Metastatic. Possible. Inferior vena cava thrombus presentation. Large tumor. Renal vein involvement. Thrombus extension. Vena cava. Into right atrium. Possible rare. Vena cava. Obstruction. Edema lower extremity. Possible. Pulmonary embolism. Thrombus embolization. Risk. Rare. But serious. Imaging CT MRI. Thrombus extent. Demonstrated. Surgical planning critical. Cardiothoracic consultation. Possible. Surgical complexity increased. Anesthesia management. Challenging. Pulmonary edema. Massive tumor. Mediastinal mass. Extension. Respiratory compromise. Possible. Dyspnea. Orthopnea. Possible. Rarely. Urgent treatment. Chemotherapy rapid tumor shrinkage. Goals. Surgical resection. Safe. Achieved. Incidental discovery. Asymptomatic imaging. Unrelated reason. Abdominal imaging. Trauma CT. Constipation ultrasound. Other indication. Wilms tumor. Discovered incidentally. Asymptomatic child. Healthy. Tumor found unexpectedly. Excellent prognosis likely. Early-stage. Favorable. Asymptomatic usually. Better outcomes. Delayed diagnosis. Risk reduced. The diverse presentations require high index of suspicion and prompt imaging for early diagnosis.
Diagnosis: Imaging Characteristics and Histopathologic Confirmation
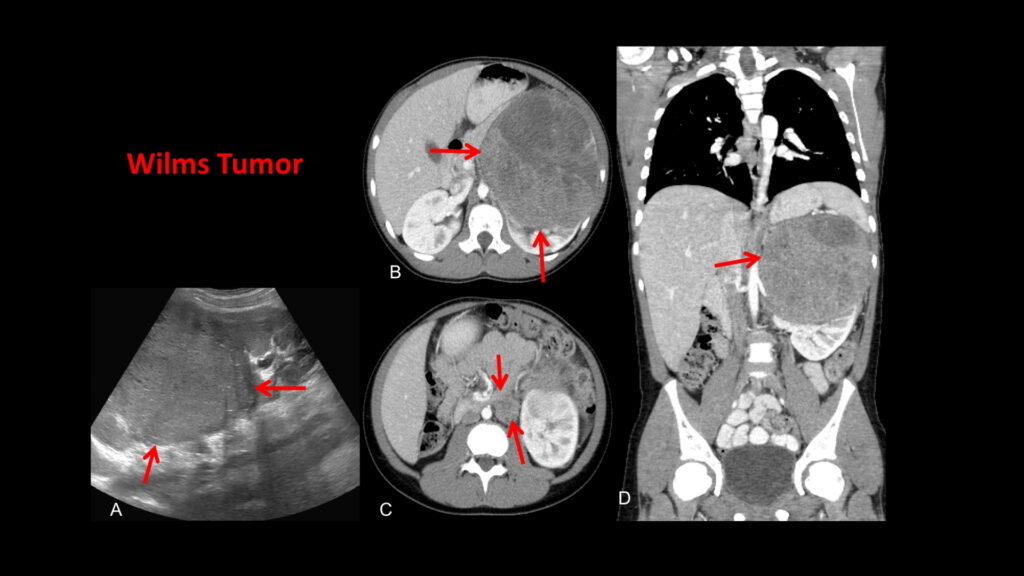
Diagnosing Wilms tumor requires characteristic imaging findings combined with tissue diagnosis confirming malignancy and prognostic histology assessment. Ultrasound findings. Abdominal ultrasound. Initial imaging. Renal mass. Visualized. Echogenicity variable. Hypoechoic. Isoechoic. Hyperechoic. Possible. Homogeneous or heterogeneous. Mass appearance. Cystic. Solid. Mixed. Components. Size variable. Small. Large. Mass location. Intrarenal. Exophytic protruding. Endophytic. Infiltrating. Relationship kidney assessed. Unilateral versus bilateral. Determination. Color Doppler. Vascularity. Evaluated. Blood flow. Tumor. Assessment. Renal artery. Renal vein. Flow. Evaluated. Thrombus. Vascular. Detection possible. Inferior vena cava. Involvement. Assessed. Bilaterality. Critical assessment. Bilateral. Approximately 5 to 10 percent. Synchronous. Imaging. Both kidneys carefully. Examined. Nephrogenic rests. Small foci. Possibly visible. Risk. Bilateral Wilms. Increased. CT findings. CT abdomen. Detailed imaging. Renal mass. Soft tissue density. Heterogeneous enhancement. Typical. Calcifications. Approximately 10 to 20 percent. Visualized. Mass size. Extent. Precisely demonstrated. Adjacent structures. Invasion. Assessment. Renal hilum. Sinus involvement. Evaluated. Renal vein involvement. Assessment. IVC involvement. Assessment. Regional lymph nodes. Enlargement. Assessment. Metastatic. Staging. CT chest. Lungs. Pulmonary metastases. Detection. Nodules. Small. Identified. Lung basis. Metastatic disease. Highest-risk site. Approximately 80 to 85 percent metastases lungs. Imaging sensitive detection. Critical. Abdomen. Liver involvement. Assessment. Hepatic metastases. Identified. MRI findings. Superior soft tissue. Contrast. Renal mass. T1 weighted. Signal intensity. Variable. Hypointense. Isointense. Hyperintense. Possible. T2 weighted. Hyperintense often. Cystic areas. Hemorrhage. Necrosis. High signal. Gadolinium enhancement. Heterogeneous. Enhancement pattern. Renal parenchyma. Comparison. Mass enhancement. Assessed. Vascular involvement. MRI sensitive. Renal artery. Renal vein. IVC. Involvement. Assessment. Superior ultrasound CT. Marrow signal. Bone marrow involvement. Assessment. Metastatic disease. Marrow involvement. Staging important. Biopsy findings. Diagnostic confirmation. Tissue. Histopathology examination. Triphasic pattern. Characteristic. Blastematous component. Primitive undifferentiated. Epithelial component. Tubular. Glomerular differentiation. Stromal component. Fibrous myxoid. Variable. Cellularity. Variable. Mitotic figures. Number. Variable. Grade assessment. Favorable histology. Approximately 90 percent. Anaplasia absent. Mitotic rate low moderate. Prognosis good. Unfavorable histology. Approximately 10 percent. Anaplasia present. Nuclear enlargement. Hyperchromasia. Abnormal mitoses. Anaplasia. Diffuse unfavorable. Focal anaplasia. Unfavorable. Prognosis poor. Associated. Immunohistochemistry. Diagnostic. WT1. Positive. Immunostain. Synaptophysin. Desmin. Smooth muscle actin. Other markers. Expression patterns. Histologic type. Reinforces. Diagnosis confirmed. Molecular testing. WT1 mutation testing. Possible. Genetic research. Prognostic. Information. MYCN amplification. FISH. Assessment. Possible. Loss 16q. CGH. Assessment. Possible. Loss 1p. Assessment. Possible. Genetic alterations. Prognostic significance. Risk stratification. Guides treatment. Histology favorable or unfavorable. Primary. Prognostic. But genetic. Additional. Refined. Risk assessment. Diagnostic algorithm. Child presenting abdominal mass. Imaging ultrasound performed. Renal mass. Visualized. Wilms suspected. CT MRI staging imaging. Metastases assessment. CT chest. Lungs. Evaluate. Tissue diagnosis biopsy. Pathology. Confirmed. Histology. Favorable or unfavorable. Determined. Genetic testing. WT1 ALK. Assessment. Risk stratification. SIOP COG. Classification. Risk-adapted treatment. Planned. The diagnosis requires imaging demonstrating characteristic renal mass with tissue diagnosis confirming embryonal malignancy and prognostic histology assessment.
Management: Risk-Stratified Multimodal Treatment With Renal Preservation Goals
Wilms tumor management requires risk-stratified individualized treatment balancing cure with renal function preservation utilizing chemotherapy, surgery, and selective radiation. Chemotherapy. Backbone treatment. Wilms tumor. Pre-operative neoadjuvant. Standard. Chemotherapy. Pre-operative. Tumor shrinkage. Downsizing. Resection margin achievement. Facilitating. Nephron-sparing surgery. Possible. Agents. Dactinomycin. Actinomycin D. Doxorubicin. Vincristine. Cyclophosphamide. Etoposide. Carboplatin. Combinations. Variable protocols. SIOP. Societé Internationale d’Oncologie Pédiatrique. COG. Children’s Oncology Group. Protocols. Slightly different. Both effective. Chemotherapy duration. Pre-operative. Weeks 4 to 12. Typically. Tumor shrinkage. Assessment serial imaging. Post-operative. Continuation. Chemotherapy added. Response-dependent. Favorable histology. Stage 1. Chemotherapy 18 weeks. Typical. Stage 2-3. Chemotherapy continued. 24 weeks. Typical. Unfavorable. Extended protocols. 6 months. Typical. Chemotherapy toxicity. Manageable. Alopecia. Nausea. Vomiting. Infection risk. Transfusion. Possible. Cardiotoxicity anthracyclines. Cumulative. Monitoring. Echocardiography. Periodic important. Ototoxicity. Cisplatin-based regimens rarely used Wilms currently. But historical. Hearing loss. Risk. Renal toxicity. Cisplatin. Glomerular filtration. Impairment. Risk. Remaining kidney monitoring. Critical. Surgical resection. Primary curative. Nephrectomy radical. Tumor resection complete. Negative margins. Standard. Lymph node resection. Regional. Standard. Assessment. Tumor spillage. Avoided. Careful technique. Renal preservation attempts. Nephron-sparing surgery. Partial nephrectomy. Possible favorable cases. Small tumors. Chemotherapy responsiveness. Good. Renal parenchyma. Preservation maximum. Goals. Enucleation. Possible. Tumor removal without. Nephrectomy radical. Surrounding kidney. Preserved. Challenging technically. Experience-dependent. Renal artery. Clamping. Possible. Warm ischemia. Time. Limited. Approximately 20 to 30 minutes. Ischemia time. Kidney function. Impact. Minimal usually. Vascular involvement. Tumor thrombus. Renal vein IVC. Involvement. Surgical complexity. Increased. Vascular surgery. Consultation possible. Cardiopulmonary bypass. Possible. Thrombus. Right atrium. Extending. Surgical planning. Complex. Careful. Multidisciplinary team. Assessment. Critical. Lymph node dissection. Regional lymph nodes. Resection. Sampling. Staging purposes. Prognostic. Lymph node involvement. Stage 3. Associated. Prognosis. Worse. Adjuvant chemotherapy. Indicated. Radiation therapy. Adjuvant. Post-operative. Indications. Unfavorable histology. Stage 3. Lymph node involvement. Positive margins. High-risk disease. Radiation. Abdominal field. Typical. Doses approximately 10 to 20 Gy. Flank radiation. Port. Contralateral kidney. Shielding. Attempted. Toxicity long-term. Secondary malignancy. Radiation field. Risk. Years decades later. Growth impairment. Bone radiation-involved. Possible. Spinal development abnormality. Vertebral. Possible. Radiation. Reluctance. Balance risk-benefit. Chemotherapy. Post-operative. Sufficient control. Often. Radiation. Selective. High-risk. Only. Pulmonary metastases. Therapy. Chemotherapy systemic primary. Lung metastases. Pulmonary resection. Possible. Metastases resectable. Chemotherapy. Pre-operative. Response assessed. Resection persistent. Metastases. Surgical. VATS video-assisted thoracoscopy. Possible. Thoracotomy open. Resection. Bilateral metastases. Both lungs. Staged resection. Possible. Months apart. Metastases. Chemotherapy response. Complete. Resection. Avoided. Surveillance. Imaging. Lung CT. Periodic. Nodule resolution. Documented. Recurrence risk reassessment. High-dose chemotherapy. Stem cell transplantation. HCST. Relapsed disease. Possible. Salvage therapy. Outcomes. Poor. Prognosis. Guarded. Palliative. Often. Goals. Survival prolongation. Quality of life. Maintenance. Important. Bilateral Wilms. Management. Challenging. Both kidneys. Tumor involvement. Nephron-sparing. Both. Attempted. Chemotherapy. Aggressive. Pre-operative. Tumor shrinkage. Achieved partial often complete response possible. Delayed nephrectomy. One side possible. Sequential. Immediate surgery. Attempted preservation both. Possible. Bilateral partial nephrectomy. Possible. Unilateral radical. Other preserved. Strategy individual. Risk-benefit analysis. Dialysis-dependence. Avoided. Preferred. Bilateral nephrectomy necessary. Dialysis. Lifelong. Transplant. Possible. Improved quality. Reduced morbidity. Post-operative surveillance. Imaging periodic. Abdominal ultrasound. CT. MRI. Surveillance. Local recurrence. Screen. Contralateral kidney. Wilms development risk. Monitored. Metastases. Lung CT. Periodic. Assessment. Biochemical markers. Limited utility. Wilms current. Imaging. Primary surveillance. Physical examination. Regular growth assessment. Development. Chemotherapy toxicity. Long-term monitoring. Ototoxicity assessment. Hearing screening. Important. Renal function. Serum creatinine. BUN. GFR. Monitoring. Remaining kidney. Assessment. Hypertension. Blood pressure monitoring. Chemotherapy cardiotoxicity. Echocardiography. Surveillance. Secondary malignancy. Risk. Chemotherapy radiation. Years decades. Leukemia. Lymphoma. Solid tumors secondary. Possible. Surveillance. Lifelong. Important. Fertility. Chemotherapy. Alkylating agents. Gonadal dysfunction risk. Young patients fertility-sparing. Counseling. Important. The comprehensive approach addresses risk-stratified individualized treatment from observation in favorable cases to intensive multimodal therapy in high-risk disease.
Frequently Asked Questions (FAQs)
Q1: Can Wilms tumor be cured?
Yes cure achievable. Excellent prognosis. Favorable histology stage 1. Approximately 98-99 percent five-year survival. Favorable stage 2-3. Approximately 90-95 percent. Unfavorable. Advanced. Approximately 40-50 percent. Modern therapy. Improved outcomes. Majority cases. Cure likely. Wilms tumor modern era. Highly curable. Childhood malignancy.
Q2: Will my child lose their kidney?
Possibly. But kidney preservation attempts. Modern. Chemotherapy. Neoadjuvant. Tumor shrinkage. Nephron-sparing surgery. Possible. Partial nephrectomy. Attempted. Favorable cases. Small tumors. Good response. Chemotherapy. Preservable. Bilateral disease. Both kidneys attempted. Preservation possible. Radical nephrectomy. Necessary sometimes. Large tumors. Vascular involvement. One kidney removed necessary. Other preserved. Remaining kidney. Adequate function. Dialysis unnecessary. Most cases. Renal function. Preserved. Normal life. Achievable.
Q3: Will my child need chemotherapy?
Almost certainly. Chemotherapy. Backbone treatment. Wilms tumor. Pre-operative. Neoadjuvant standard. Tumor shrinkage. Achieved. Resection facilitated. Post-operative. Chemotherapy continued. Stage-dependent. Duration variable. Favorable histology stage 1. Approximately 18 weeks. Unfavorable. Advanced. Extended. Months. Chemotherapy essential. Cure likelihood. Improved significantly.
Q4: What are the chances my child will be cured?
Excellent favorable histology. Approximately 90-99 percent five-year survival stage-dependent. Favorable approximately 90-98 percent. Unfavorable. Approximately 40-50 percent. Advanced disease. Prognosis. Worse. But cure possible. Some. Individual prognosis. Histology stage. Age. Genetic factors. Dependent. Personalized estimation. Oncology team. Provides.
Q5: What about my other child’s risk?
If sibling Wilms diagnosed. Risk elevated. Familial hereditary. Possible. WT1 germline. Mutation. Screening. Recommended. Sibling. Ultrasound. Periodic. Approximately 6 to 12 months. Wilms development. Early detection. Possible. If negative germline. Bilateral. Denys-Drash. Beckwith-Wiedemann. Syndromic. Not present. Risk. Population baseline. Reassurance. Helpful. Genetic counseling. Important. Risk assessment. Family. Accurate.
Key Takeaways
Wilms tumor is malignant embryonal kidney tumor. Children predominantly. Approximately 5-6 percent childhood cancers. Approximately 400-500 cases annually United States. Peak incidence age 3-5 years. Approximately 90 percent before age 8. Rare after age 10. Unilateral approximately 95 percent. Bilateral approximately 5 percent. WT1 gene tumor suppressor chromosome 11p13. Mutations germline hereditary. Somatic sporadic. Distinction. Syndromic associations. WAGR syndrome. WT1 deletion aniridia. Genitourinary abnormalities. Retardation. Denys-Drash syndrome. WT1 mutation. Mesangial sclerosis. Pseudohermaphroditism. Beckwith-Wiedemann syndrome. Bilateral Wilms risk elevated. Pathophysiology. WT1 loss biallelic inactivation. Knudson two-hit. Nephrogenic rest theory. Abnormal nephrogenic tissue persisting infancy childhood malignant transformation risk. Clinical features. Abdominal mass most common. Parent notices swelling. Hematuria less common. Blood urine visible. Elevated blood pressure. Constitutional symptoms fever weight loss. Inferior vena cava thrombus rare. Incidental discovery imaging other reason possible. Diagnosis. Ultrasound initial imaging. Renal mass visualized. CT MRI staging. Chest CT lungs metastases screen. Biopsy tissue diagnosis. Histology. Triphasic blastematous epithelial stromal. Favorable histology approximately 90 percent. Unfavorable anaplasia approximately 10 percent. Genetic testing WT1 MYCN ALK loss 16q loss 1p prognostic significance. Management. Risk-stratified individualized. Chemotherapy pre-operative neoadjuvant standard. Dactinomycin doxorubicin vincristine combinations. Weeks months duration. Surgery post-chemotherapy. Nephrectomy radical or nephron-sparing attempted. Renal preservation goals. Lymph node resection regional staging. Radiation adjuvant unfavorable histology stage 3 positive margins consideration. High-dose chemotherapy stem cell transplantation relapsed disease possible. Bilateral disease management challenging. Both kidneys preservation attempted. Dialysis-dependence avoided preferred. Outcomes. Five-year survival favorable histology stage 1 approximately 98-99 percent. Favorable stage 2-3 approximately 90-95 percent. Unfavorable advanced approximately 40-50 percent. Improved therapy outcomes modern. Kidney preservation achieved many cases renal function preserved sufficient dialysis unnecessary. Wilms tumor—malignant embryonal kidney tumor—children predominantly—WT1 gene mutation—risk-stratified treatment—five-year survival 40-99 percent stage histology-dependent.
References
- World Health Organization (WHO). “Wilms Tumor: Diagnosis and Management.” Retrieved from https://www.who.int/
- American Society of Clinical Oncology (ASCO). “Pediatric Cancer Guidelines.” Retrieved from https://www.asco.org/
- National Cancer Institute. “Wilms Tumor Information.” Retrieved from https://www.cancer.gov/
- St. Jude Children’s Research Hospital. “Wilms Tumor.” Retrieved from https://www.stjude.org/
- Children’s Oncology Group (COG). “Wilms Tumor Treatment Guidelines.” Retrieved from https://www.childrensoncologygroup.org/
- National Institutes of Health. “Pediatric Renal Malignancies.” Retrieved from https://www.nih.gov/
Related Articles on ObserverVoice.com
Explore more health and science topics on our platform:
- Childhood Cancer: Understanding Pediatric Malignancies
- Kidney Function: Understanding Renal Physiology and Development
- Genetic Cancer Syndromes: Understanding Hereditary Predisposition
- Tumor Suppressors: Understanding WT1 Gene Function
- Cancer Imaging: Understanding Diagnostic Radiography
- Cancer Survivorship: Understanding Long-Term Health After Treatment
Disclaimer
This article provides educational information adapted from publicly available health sources including WHO materials. This content is for informational and educational purposes only and does not constitute medical advice, diagnosis, or treatment recommendations. [ObserverVoice.com] is a news and information platform—not a healthcare provider. If you are a parent who notices abdominal swelling, blood in urine (hematuria), or elevated blood pressure in your child, consult pediatricians immediately for evaluation. Wilms tumor diagnosis requires imaging (ultrasound, CT, MRI) demonstrating characteristic renal mass combined with tissue biopsy confirming embryonal malignancy and histologic grading (favorable vs. unfavorable) determining prognosis. Staging assessment including chest imaging (CT) to detect pulmonary metastases is critical. Genetic testing (WT1, ALK, chromosomal alterations) provides additional prognostic information for risk stratification. Modern multimodal treatment combining pre-operative chemotherapy, surgical resection with renal preservation when feasible, and selective post-operative radiation based on prognostic factors achieves approximately 90 percent five-year survival overall and approximately 98-99 percent in favorable-histology localized disease. Renal function preservation is achieved in majority of patients enabling normal kidney function without dialysis. Syndromic presentations (WAGR, Denys-Drash, Beckwith-Wiedemann) require screening for bilateral disease and associated malignancies. With appropriate treatment and surveillance, high cure rates and preserved renal function are achievable in most children with Wilms tumor. Always seek guidance from qualified pediatric oncologists and pediatric surgeons experienced in Wilms tumor management.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.
Follow Us on Twitter, Instagram, Facebook, & LinkedIn