
Type 1 Diabetes: Autoimmune Destruction of the Pancreas From Day One
Type 1 Diabetes is a chronic autoimmune disease in which the immune system attacks and destroys the insulin-producing cells in the pancreas. The destroyed cells are beta cells located in the islets of Langerhans within the pancreas. Insulin is a hormone essential for blood glucose regulation. Insulin allows cells to take up glucose from the blood. Without insulin, glucose accumulates in the blood. Blood glucose becomes dangerously high. Severe complications develop. Type 1 Diabetes is characterized by insulin deficiency. The body produces little or no insulin. Without insulin treatment, Type 1 Diabetes is fatal. Insulin therapy is essential. Unlike Type 2 Diabetes which results from insulin resistance, Type 1 Diabetes results from immune destruction of insulin-producing cells. The distinction is crucial. Type 1 Diabetes requires insulin replacement. Type 2 Diabetes is managed differently. Type 1 Diabetes affects approximately five to ten million people worldwide. The disease is the most common form of diabetes in children. Type 1 Diabetes accounts for approximately five to ten percent of all diabetes cases. The disease typically develops in children and young adults. Most commonly diagnosed before age twenty years. However, Type 1 Diabetes can develop at any age. LADA, or latent autoimmune diabetes in adults, develops more slowly in older individuals. Type 1 Diabetes develops equally in males and females. Slightly more common in Caucasians than other ethnicities. Type 1 Diabetes is caused by abnormal immune activation against beta cells. B cells produce autoimmune antibodies against insulin. Antibodies against glutamic acid decarboxylase, or GAD. Antibodies against insulin. Antibodies against zinc transporter eight, or ZnT8. T cells infiltrate pancreatic islets. The immune attack gradually destroys beta cells. Beta cells are progressively eliminated. Insulin production decreases. Eventually, ninety percent or more of beta cells are destroyed. Insulin production becomes insufficient. Hyperglycemia develops. Severe hyperglycemia causes symptoms. Early diagnosis and immediate insulin treatment are crucial for preventing severe complications and achieving good long-term control. With modern insulin regimens and glucose monitoring, people with Type 1 Diabetes can achieve excellent glycemic control. Many achieve near-normal blood glucose levels. Complications can be prevented or delayed. Understanding Type 1 Diabetes helps with early recognition and appropriate management to prevent serious complications.
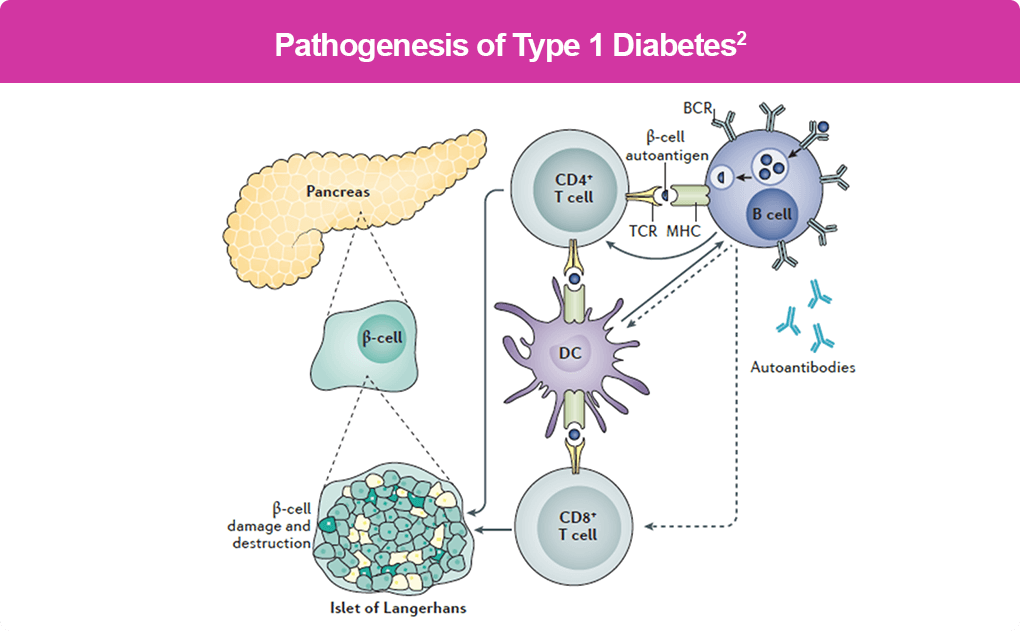
How Does Immune Attack on Beta Cells Cause Type 1 Diabetes?
To understand Type 1 Diabetes, we need to learn about the pancreas, beta cells, and the immune system. The pancreas is an endocrine gland located in the abdomen. The pancreas produces insulin. Insulin is essential for glucose metabolism. The islets of Langerhans contain the insulin-producing cells. Beta cells produce insulin. The pancreas also produces glucagon. Glucagon raises blood glucose. The pancreas also produces other hormones. Insulin allows glucose uptake by cells. Glucose is used for energy. Without insulin, cells cannot take up glucose. Glucose accumulates in blood. Hyperglycemia develops. In Type 1 Diabetes, the immune system becomes abnormally activated. B cells produce autoimmune antibodies. Anti-insulin antibodies develop. Anti-GAD antibodies develop. Anti-ZnT8 antibodies develop. These antibodies specifically target beta cells. The antibodies bind to beta cell antigens. Complement is activated. Inflammation occurs. Beta cells are damaged. T cells infiltrate pancreatic islets. CD8 positive T cells attack beta cells directly. CD4 positive T cells help coordinate immune response. Inflammatory cytokines are produced. Interleukin-2, interleukin-6, TNF-alpha increase. These inflammatory mediators activate more immune cells. The inflammation spreads throughout islets. Beta cells are progressively destroyed. The destruction is gradual. Early Type 1 Diabetes shows immune infiltration of islets. Lymphocytes infiltrate. Inflammation present. However, beta cells still present. Beta cell function still partially preserved. Progressive Type 1 Diabetes shows increasing beta cell loss. Advanced Type 1 Diabetes shows extensive beta cell destruction. Ninety percent or more of beta cells destroyed. Few beta cells remain. Insulin production severely reduced. Severe hyperglycemia occurs. The inflammatory process is progressive. The beta cell destruction occurs over weeks to months. In children, often rapid. Symptoms develop suddenly. In adults, often slower. LADA develops gradually. The progression varies between individuals. Some progress rapidly to complete beta cell failure. Others retain some beta cell function. Residual beta cell function may persist. Some produce small amounts of insulin. This residual function may slow complications. However, insulin treatment required. The systemic nature of Type 1 Diabetes. It is an autoimmune disease. Other autoimmune diseases may coexist. Celiac disease. Hashimoto’s thyroiditis. Graves’ disease. Addison’s disease. Type 1 Diabetes appears with other autoimmune diseases. Polyautoimmunity. Multiple autoimmune diseases. Complex management needed. Understanding the immune mechanisms has led to development of effective insulin replacement and management strategies.
What Are the Main Symptoms and Signs of Type 1 Diabetes?
Type 1 Diabetes causes multiple symptoms from severe hyperglycemia and its metabolic consequences. The symptoms develop acutely in most cases. Polyuria, or excessive urination. Frequent urination. Increased volume. Day and night. Nocturia. Waking at night to urinate. Bedwetting in children. Previously toilet-trained children may develop enuresis. Frequent and urgent urination throughout day. Polydipsia, or excessive thirst. Intense thirst. Excessive drinking. Polydipsia. Extreme thirst unrelenting. Drives seeking fluids. Polyphagia, or excessive hunger. Increased appetite. Despite eating more, weight loss occurs. Hunger despite recent eating. Fatigue. Profound exhaustion. Weakness. Lethargy. Difficulty with normal activities. Severe fatigue. Weight loss despite increased appetite. Progressive weight loss. Rapid onset. Loss of muscle mass. Fat loss. Noticeable change in appearance. Irritability. Mood changes. Behavioral changes. Irritability and mood swings. Depression or anxiety. Confusion. Mental changes in children. Difficulty concentrating. School performance decline. Behavioral problems at school. Blurred vision. Vision changes. Difficulty focusing. Blurry vision. Light-headedness or dizziness. Feeling faint. Vertigo. Unsteadiness. Fruity-smelling breath. Acetone smell. Distinctive fruity odor. Sign of ketoacidosis. Nausea and vomiting. Abdominal pain. Stomach discomfort. Cramping. May mimic appendicitis or other acute abdomen. Rapid breathing. Hyperventilation. Increased respiratory rate. Kussmaul breathing. Deep, labored breathing. Sign of metabolic acidosis. Diabetic ketoacidosis signs. Life-threatening emergency. Ketoacidosis develops rapidly. Hyperglycemia causes osmotic diuresis. Dehydration occurs. Electrolyte imbalance. Metabolic acidosis. Altered mental status. Confusion progressing to coma. Shock. Cardiovascular collapse. Risk of death. DKA is medical emergency. Requires immediate hospitalization. Insulin therapy. Fluids. Electrolyte correction. Intensive care monitoring. Early symptoms may be nonspecific. Fatigue attributed to other causes. Irritability assumed to be behavioral. Increased urination thought normal. Weight loss attributed to growth. Progressive recognition of pattern. Multiple symptoms together. Rapid onset prompts evaluation. Classic presentation. Rapid onset with multiple symptoms. Medical evaluation. Laboratory testing. Early diagnosis prevents DKA. Immediate insulin treatment prevents severe complications.
How is Type 1 Diabetes Detected and Diagnosed?
Type 1 Diabetes is diagnosed through laboratory tests measuring blood glucose and confirming autoimmunity. Early diagnosis is critical. Clinical history is important. Polyuria and polydipsia. Polyphagia with weight loss. Fatigue. Irritability. Vision changes. Fruity-smelling breath if DKA. Family history of diabetes. Coexisting autoimmune diseases. Physical examination reveals characteristic findings. Weight loss. Dehydration. Fruity-smelling breath. Rapid breathing if DKA. Altered mental status if DKA. Fasting blood glucose. Fasting glucose greater than one hundred twenty-six milligrams per deciliter indicates diabetes. Random blood glucose. Greater than two hundred milligrams per deciliter with symptoms diagnostic. Two-hour postload glucose. Following one hundred twenty-five gram glucose drink. Greater than two hundred indicates diabetes. Hemoglobin A1C. Measures average glucose over three months. A1C greater than six point five percent indicates diabetes. Reflects glycemic control over time. Used for monitoring. Venous plasma glucose. Gold standard for diagnosis. Oral glucose tolerance test. Rarely used for Type 1. Used more for Type 2. Autoimmune markers. Anti-GAD antibodies. Present in most Type 1 patients. Support autoimmune diagnosis. Anti-insulin antibodies. Present in many Type 1 patients. Support autoimmune diagnosis. Anti-ZnT8 antibodies. Present in many Type 1 patients. Support autoimmune diagnosis. C-peptide level. Measures endogenous insulin production. Reduced in Type 1. Higher in Type 2. Helps distinguish Type 1 from Type 2. Fasting C-peptide. Low or undetectable indicates beta cell failure. Urine ketones. Positive if ketoacidosis present. Urinalysis. Tests for glucose in urine. Glycosuria indicates hyperglycemia exceeding renal threshold. Tests for ketones. Ketonuria indicates ketoacidosis. Serum electrolytes. Potassium, sodium, chloride, bicarbonate. Electrolyte imbalance if DKA. Venous or arterial pH. Low pH indicates metabolic acidosis. If DKA present. Blood glucose trending. Multiple glucose measurements. If newly diagnosed. Assess severity. Assess need for hospitalization. Complete blood count. Usually normal. Infection screening if DKA. Metabolic panel. Kidney function. Liver function. Baseline assessment. Screen for coexisting conditions. Screen for other autoimmune diseases. Celiac serology. Thyroid function. Check for coexisting autoimmune thyroiditis. The combination of clinical presentation with fasting glucose greater than one hundred twenty-six, random glucose greater than two hundred with symptoms, elevated A1C, positive autoimmune antibodies, and reduced C-peptide confirms Type 1 Diabetes diagnosis. Early diagnosis allows immediate insulin treatment. Diagnostic delay risks DKA.
What Health Complications Do People with Type 1 Diabetes Face?
People with Type 1 Diabetes face serious acute and chronic complications from hyperglycemia and its metabolic effects. The complications depend on glycemic control and disease duration. Diabetic ketoacidosis is the most serious acute complication. Severe hyperglycemia. Metabolic acidosis. Dehydration. Electrolyte imbalance. Life-threatening emergency. Altered mental status progressing to coma. Shock. Cardiovascular collapse. Mortality high without urgent treatment. Occurs at diagnosis in some. Occurs during illness or stress. Inadequate insulin therapy. Infection triggering DKA. DKA prevention through insulin compliance essential. Hypoglycemia. Low blood glucose. Blood glucose less than seventy milligrams per deciliter. Adrenergic symptoms. Trembling. Sweating. Palpitations. Anxiety. Neuroglycopenic symptoms. Confusion. Difficulty concentrating. Slurred speech. Altered behavior. Loss of consciousness. Seizure. Hypoglycemic coma. Severe hypoglycemia can cause brain damage. Death if not treated. Frequent severe hypoglycemia increases risk of complications. Hypoglycemia unawareness develops. Loss of warning symptoms. Dangerous. Hyperglycemia. Persistent high blood glucose. Causes symptoms. Increases risk of complications. Accelerates long-term complications. Microvascular complications. Retinopathy. Damage to retina. Vision loss. Blindness. Leading cause of blindness in working-age adults. Nephropathy. Kidney damage. Progressive kidney function loss. Proteinuria. Hematuria. Hypertension. End-stage renal disease. Kidney transplant. Dialysis. Neuropathy. Nerve damage. Peripheral neuropathy. Numbness. Tingling. Pain. Sensory loss. Increased foot injury risk. Autonomic neuropathy. Bowel dysfunction. Bladder dysfunction. Sexual dysfunction. Cardiovascular dysfunction. Gastroparesis. Delayed gastric emptying. Abdominal discomfort. Nausea. Vomiting. Nutritional problems. Macrovascular complications. Coronary artery disease. Myocardial infarction. Heart attack. Young age at onset. Accelerated atherosclerosis. Stroke. Cerebrovascular disease. Peripheral vascular disease. Amputation. Foot disease. Diabetic foot ulcers. Infection. Osteomyelitis. Gangrene. Amputation. Major source of disability and mortality. Hypertension. Blood pressure elevation. Accelerated by hyperglycemia. Kidney disease. Cardiovascular disease. Dyslipidemia. Lipid abnormalities. Elevated LDL cholesterol. Elevated triglycerides. Reduced HDL cholesterol. Cardiovascular disease risk. Depression. Mood disorders. Depression common. Anxiety. Emotional burden of chronic disease. Mental health support important. Eating disorders. Disordered eating. Insulin omission for weight loss. Dangerous. Diabulimia. Accelerates complications. Bone health. Increased fracture risk. Osteoporosis. Diabetic osteoarthropathy. Frozen shoulder. Limited joint mobility. Infections. Increased infection risk. Hyperglycemia impairs immune function. Urinary tract infections. Skin infections. Periodontal disease. Dental health complications. Associated autoimmune diseases. Celiac disease. Malabsorption. Nutritional deficiency. Thyroid disease. Hypothyroidism or Graves’ disease. Addison’s disease. Electrolyte abnormalities. Polyautoimmunity. Without adequate insulin therapy and glycemic control, complications rapidly develop. With appropriate insulin therapy and good glycemic control, many complications preventable or delayed.
What Treatments Help People with Type 1 Diabetes?
Treatment for Type 1 Diabetes focuses on insulin replacement and maintaining near-normal blood glucose levels. Insulin therapy is essential. No alternative treatment. Insulin is necessary for survival. Multiple insulin formulations available. Rapid-acting insulins. Insulin lispro. Insulin aspart. Insulin glulisine. Action begins within minutes. Peak action thirty to ninety minutes. Duration two to four hours. Used at mealtimes. Short-acting insulins. Regular insulin. Action begins within thirty minutes. Peak action two to four hours. Duration six to eight hours. Less commonly used. Intermediate-acting insulins. NPH insulin. Action begins one to two hours. Peak action four to eight hours. Duration twelve to sixteen hours. Used for basal insulin. Long-acting insulins. Insulin glargine. Insulin detemir. Insulin degludec. Action begins one to two hours. Minimal peak. Steady action throughout day. Duration twenty to forty-two hours. Used for basal insulin. Ultra-long-acting insulins. Insulin degludec. Extended duration. Steady glucose levels. Combination insulins. Pre-mixed insulins. Rapid-acting and intermediate-acting combined. Fixed ratios. Less flexible. Used less commonly. Insulin delivery methods. Insulin injections. Multiple daily injections. MDI therapy. Basal-bolus regimen. Basal insulin once or twice daily. Bolus insulin at meals. Flexible. Insulin pumps. Continuous insulin infusion. CSII. Programmable. Infuses insulin continuously. Boluses at meals. More physiologic. Better glycemic control in many. Insulin pens. More convenient than vials and syringes. Pre-filled. Reusable or disposable. Inhalation insulin. Afrezza. Rapid-acting. Inhaled at meals. Oral inhalers. Alternative for some. Glucose monitoring. Self-monitoring of blood glucose. SMBG. Fingerstick checks. Multiple daily. Before meals. Before bed. When hypoglycemic. Guides insulin dosing. Continuous glucose monitoring. CGM. Sensor under skin. Real-time glucose readings. Alerts for high and low glucose. Improved glycemic control. Reduced hypoglycemia. Integration with pumps. Automated insulin delivery. Hypoglycemia treatment. Rapid-acting carbohydrates. Glucose tablets. Fruit juice. Candy. Raise blood glucose fifteen grams carbohydrate. Recheck in fifteen minutes. Repeat if still low. Glucagon. Intramuscular injection for severe hypoglycemia. Raises blood glucose. Emergency treatment. Others should know how to give. Glucagon nasal spray available. Easier to administer. Medical evaluation and support. Endocrinologist. Diabetes specialist. Diabetes educator. Nutritionist. Regular follow-up. HbA1c monitoring. Quarterly or annually. Complication screening. Annual eye exam. Annual urine protein check. Annual foot exam. Blood pressure monitoring. Lipid monitoring. Annual. More frequently if abnormal. Kidney function monitoring. Annual creatinine. Annual urine protein. Psychological support. Diabetes distress. Depression screening. Counseling if needed. Continuous improvement of insulin regimens. Aim for HbA1c less than seven percent. Some target less than six point five percent. Individualized goals. Avoid severe hypoglycemia. Exercise within tolerance. Regular physical activity. Reduces insulin requirements. Improves cardiovascular health. Reduces complications. Nutrition management. Carbohydrate counting. Calculate insulin dose based on carbohydrate content. Balanced diet. Adequate protein. Adequate fat. Limit added sugars. Limit processed foods. Weight management if overweight. With appropriate insulin therapy, frequent glucose monitoring, and good glycemic control, people with Type 1 Diabetes achieve excellent health outcomes. Complications significantly reduced or prevented.
Living with Type 1 Diabetes
Living with Type 1 Diabetes requires daily insulin management, glucose monitoring, lifestyle modifications, and psychological adjustment to a chronic disease requiring constant self-care. For people newly diagnosed with Type 1 Diabetes, the diagnosis is overwhelming. Learning about a disease requiring lifelong insulin is frightening. Risk of severe complications. Intensive self-management required. However, understanding that effective insulin therapy exists and good control is achievable offers hope. Patient education about Type 1 Diabetes, insulin management, glucose monitoring, and disease course helps people understand their condition. Understanding intensive management prevents complications. Insulin administration compliance is absolutely essential. Insulin injections or pump use. Consistent timing. Dose adjustment for meals. Dose adjustment for activity. Failure to take insulin causes hyperglycemia. DKA risk. Dangerous. Insulin therapy cannot be missed. Glucose monitoring discipline. Regular fingerstick checks. Or continuous glucose monitoring. Multiple daily checks. Especially important initially. As experience builds, frequency may decrease. However, frequent monitoring essential. Guides insulin dosing. Recognizes patterns. Detects hypoglycemia. Carbohydrate counting and meal planning. Learning carbohydrate content of foods. Calculating insulin dose for meals. Balanced nutrition. Insulin-to-carbohydrate ratio. Individualized. Adjusted based on experience. Complex skills. Diabetes educator helps. Blood glucose target. Usually seventy to one hundred eighty milligrams per deciliter. Goal HbA1c less than seven percent. Some target lower. Individualized targets. Pre-meal glucose. Bedtime glucose. Early morning glucose. Activity management. Exercise affects glucose. Increases insulin sensitivity. May cause hypoglycemia. Careful glucose monitoring needed. Plan ahead. Carry fast-acting carbohydrates. Post-exercise hyperglycemia. May occur hours after exercise. Monitor. Adjust insulin. Stress management. Stress increases blood glucose. Elevated cortisol. Elevated epinephrine. Hyperglycemia. Stress reduction. Meditation. Yoga. Regular exercise. Counseling. Reduces stress. Reduces hyperglycemia. Sleep quality. Poor sleep increases insulin resistance. Hyperglycemia. Regular sleep schedule. Adequate sleep duration. Sleep quality. Work and school adjustments. Frequent glucose checks needed. Hypoglycemia risk. Needs snacks available. Flexible schedule. Medical appointments frequent initially. Or if poorly controlled. Some need more frequent checks. School-age children. Glucose checks at school. Insulin administration at school. Nurse assistance. Individualized education plans. IEPs. Allow management needs. Teachers understanding. Peer education. Reduced stigma. Nutrition management. Balanced diet. Adequate calories. Growth and development. Especially important in children. Carbohydrate-consistent diet. Simplified counting. Meal planning support. Nutritionist guidance. Family involvement. Family understanding of disease. Support with management. Encouragement. Emotional support. Dating and relationships. Explaining condition to partners. Device visibility. Pump, CGM. Insulin injections. Partner understanding. Sexual function. Usually preserved. Reduced if complications. Sexual dysfunction from autonomic neuropathy. Communication helps. Pregnancy planning. Type 1 Diabetes pregnancy possible. Requires careful planning. Intensive glucose monitoring. Tight control important. HbA1c less than six point five percent before pregnancy. Reduces birth defects. Glucose control throughout pregnancy essential. Fetal monitoring. More frequent prenatal care. Usually successful pregnancies. Insulin requirements may increase during pregnancy. Mental health support crucial. Diabetes distress. Overwhelming daily demands. Fear of complications. Anxiety. Depression. Counseling helps. Support groups. Others with Type 1 Diabetes. Share experiences. Coping strategies. Online communities. Social support from family and friends. Family education about disease. Understanding hypoglycemia emergency. How to administer glucagon. Support with daily management. Emotional support crucial. Regular medical follow-up. Endocrinologist visits. Quarterly or more frequently. HbA1c monitoring. Quarterly or annually. Complication screening. Annual. More frequently if abnormal. Adjustment of insulin regimens. Based on HbA1c and glucose patterns. Individualization. Preventing complications. With appropriate insulin therapy ensuring consistent daily administration, frequent glucose monitoring guiding insulin dosing, carbohydrate counting for meal insulin, stress management, adequate sleep, exercise within tolerance, nutrition management, psychological support, family and social support, most people with Type 1 Diabetes achieve good glycemic control and maintain excellent quality of life and prevent serious complications with appropriate lifelong insulin management and self-care.
Frequently Asked Questions About Type 1 Diabetes
FAQ 1: Can Type 1 Diabetes be prevented? Type 1 Diabetes cannot be prevented currently. Genetic predisposition cannot be changed. However, research ongoing. Beta cell regeneration therapies. Immune tolerance induction. Potential future prevention. Currently, no proven prevention. For those with genetic risk, no intervention prevents disease. Early diagnosis allows early treatment. Better outcomes with early insulin therapy.
FAQ 2: Is Type 1 Diabetes curable? Type 1 Diabetes cannot be cured currently. Beta cell destruction permanent. Beta cell regeneration not yet possible. However, treatment highly effective. Insulin therapy restores normal glucose metabolism. Good glucose control prevents complications. Quality of life excellent with proper management. Research ongoing. Stem cell therapy. Beta cell transplantation. Pancreas transplantation. Potential future cures. However, currently not available.
FAQ 3: Can Type 1 Diabetes be cured with a pancreas transplant? Pancreas transplant can cure Type 1 Diabetes. New pancreas produces insulin. No insulin needed. However, transplant surgery serious. Immunosuppression required. Risks exceed benefit in many cases. Reserved for kidney transplant patients. Kidney-pancreas transplants. Or life-threatening complications. However, successful transplants give insulin independence. Excellent long-term outcomes in appropriate candidates.
FAQ 4: What is the life expectancy for people with Type 1 Diabetes? Life expectancy near normal with good glycemic control. Studies show near-normal lifespans. Excellent care. Good compliance. People with Type 1 live into their eighties and nineties. However, poorly controlled diabetes reduces life expectancy. Complications shorten life. However, with modern insulin and management, prognosis excellent. Most live normal or near-normal lifespans.
FAQ 5: Are there new treatments being developed for Type 1 Diabetes? Yes, significant research ongoing. Closed-loop insulin systems. Artificial pancreas. Combines glucose monitor with insulin pump. Automated insulin delivery. Reduces hypoglycemia. Improves glucose control. FDA approval expected. Beta cell regeneration. Stem cell therapy. Growth factors stimulating beta cell production. Phase testing. JAK inhibitors. Slowing immune attack on beta cells. Phase studies. Tolerance induction. Restoring immune tolerance. Preventing beta cell attack. Early testing. Pancreatic islet transplantation. From deceased donors. Into liver. Beta cells produce insulin. Immunosuppression required. But successful in many. Advances ongoing. Better treatments anticipated.
References and Further Reading
For more information about Type 1 Diabetes, you can visit several trusted and authoritative sources providing detailed information for patients and families dealing with this autoimmune disease. The World Health Organization at WHO.int provides comprehensive information about Type 1 Diabetes and autoimmune destruction of beta cells. The American Diabetes Association at Diabetes.org offers excellent patient education, family resources, and comprehensive information about Type 1 Diabetes management. JDRF at JDRF.org provides patient education and supports research for Type 1 Diabetes cure. The American Association of Diabetes Educators at AADE.org provides resources about diabetes education and management. MedlinePlus, a service of the National Library of Medicine at MedlinePlus.gov, has detailed medical information about Type 1 Diabetes written in language that patients and families can easily understand without specialized medical knowledge. The five main reference links are: 1) WHO.int – Type 1 Diabetes, 2) American Diabetes Association, 3) JDRF, 4) American Association of Diabetes Educators, and 5) MedlinePlus – Type 1 Diabetes.
Disclaimer
This article adapts publicly available information from WHO’s Type 1 Diabetes and autoimmune destruction information pages. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform — not a healthcare provider. If you or someone you know has been diagnosed with Type 1 Diabetes or shows signs of this condition including polyuria, polydipsia, polyphagia with weight loss, fatigue, irritability, vision changes, fruity-smelling breath, or other symptoms of hyperglycemia, please consult immediately with qualified healthcare professionals, endocrinologists, and diabetes specialists for proper diagnostic evaluation with fasting glucose, random glucose, A1C, and autoimmune antibody testing, and for immediate insulin therapy initiation and diabetes education. Early diagnosis and early appropriate insulin therapy prevent diabetic ketoacidosis and severe complications. Regular glucose monitoring and insulin management are essential for preventing long-term complications. For more information, visit WHO.int and ObserverVoice.com.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.