
Social Determinants of Health: Why Your ZIP Code Matters More Than Your Genetic Code
Key Facts
- Social determinants of health cause health inequities responsible for avoidable differences in life expectancy exceeding 20 years between and within countries, according to WHO
- Children born in high-income countries can expect to live 18 years longer on average than those born in low-income countries—a gap attributable primarily to social conditions rather than biology
- WHO reports that health systems account for only 10-20% of health outcomes, while social determinants including education, income, and environment drive 80-90%
- An estimated 14 million deaths annually—roughly 25% of all global deaths—are attributable to social and economic inequalities
- People with less than 12 years of education die on average 9 years younger than those completing higher education, controlling for other factors.
When WHO’s Commission on Social Determinants of Health released its landmark 2008 report “Closing the Gap in a Generation,” it made a provocative declaration: the circumstances in which people are born, grow, live, work, and age—not primarily genetics or personal choices—determine health outcomes, and systematic differences in these circumstances create health inequities that kill millions unnecessarily. The Commission documented that social injustice literally kills on a grand scale, with poverty, discrimination, lack of education, poor housing, and unemployment acting as fundamental causes of disease that medical interventions alone can never overcome. WHO’s updated 2024 framework recognizes these patterns have intensified: the COVID-19 pandemic exposed and exacerbated existing inequities, with marginalized populations experiencing disproportionate infection, severity, and economic devastation. This article examines WHO’s comprehensive analysis of social determinants: what they are, how they shape health across populations, why addressing them requires action far beyond the health sector, and why these health initiatives represent the most consequential yet politically challenging frontier in global health equity.
What Are Social Determinants of Health? — WHO’s Definition
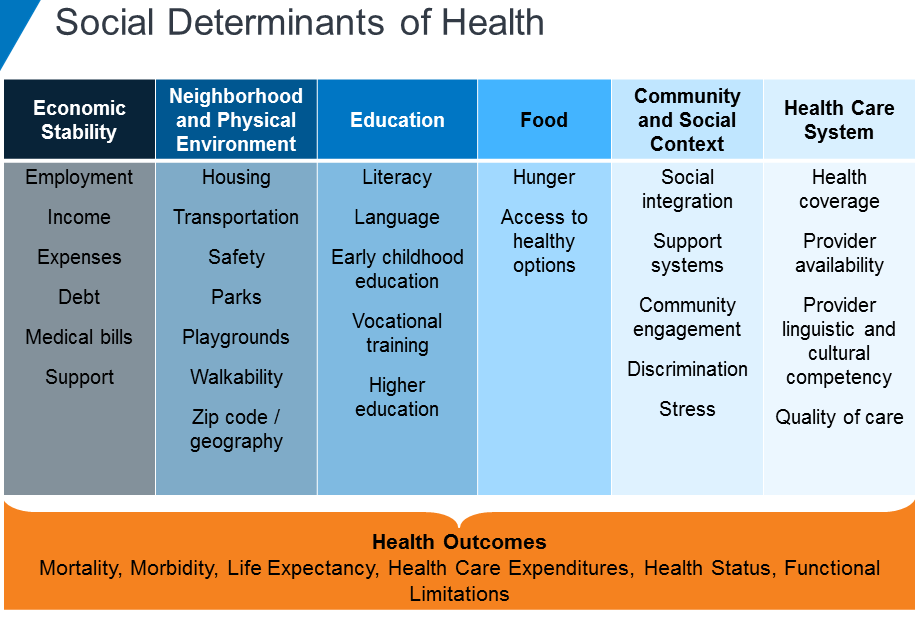
According to WHO, social determinants of health are the conditions in the environments where people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks. WHO’s framework defines these determinants as shaped by the distribution of money, power, and resources at global, national, and local levels, which are themselves influenced by policy choices. The organization emphasizes that social determinants are largely responsible for health inequities—the unfair and avoidable differences in health status seen within and between countries.
WHO categorizes social determinants into structural determinants and intermediary determinants. Structural determinants include socioeconomic position determined by income, education, occupation, social class, gender, and race/ethnicity; the broader context of governance, macroeconomic policies, social policies, cultural and societal values; and the distribution of power and resources within society. These create social stratification—the hierarchical ordering of society into groups with differential access to resources and opportunities.
Intermediary determinants include material circumstances (living conditions, working conditions, food availability); psychosocial circumstances (stressful living conditions, social support networks); behavioral and biological factors influenced by social context rather than purely individual choice; and the health system itself as a social determinant—access, quality, and responsiveness of healthcare. WHO stresses that these intermediary factors are themselves shaped by structural determinants, creating pathways through which social position affects health.
The framework deliberately positions health as more than an individual responsibility—it’s a social outcome produced by societal organization. This perspective challenges individualistic approaches blaming poor health on personal choices while ignoring that choices occur within constraints created by social position. Can someone “choose” healthy food when grocery stores don’t exist in their neighborhood? Can they “choose” exercise when their community lacks safe parks and they work multiple jobs leaving no time? WHO’s model recognizes that systematic differences in the conditions of daily life create systematic health differences that medical care alone cannot eliminate.
Global Burden
WHO documents that social determinants create health inequities resulting in avoidable differences in life expectancy, disease burden, and quality of life that vary dramatically both between and within countries. According to WHO’s health equity monitoring data, children born in low-income countries have a life expectancy at birth of approximately 63 years, compared to 81 years in high-income countries—an 18-year gap attributable primarily to social conditions including poverty, malnutrition, unsafe water, inadequate sanitation, and limited healthcare access rather than genetic or biological differences.
Within countries, inequities often exceed those between countries. In the United States, life expectancy varies by more than 20 years between the wealthiest and poorest counties. Japanese urban-rural disparities show 5-6 year gaps. Indian caste-based health inequities persist across generations despite legal protections. These within-country gaps demonstrate that national wealth doesn’t ensure equitable health—distribution of resources and opportunities matters more than aggregate prosperity.
Education gradients in health prove remarkably consistent globally. Research published in The Lancet documents that people with less than 12 years of education die on average 9 years younger than those completing higher education, after controlling for income, occupation, and other factors. Education affects health through multiple pathways: enabling better-paying stable employment, increasing health literacy and navigation of healthcare systems, expanding social networks providing support, and conferring social status that buffers against stressors.
Income-based health disparities operate at individual and societal levels. WHO reports that within countries, each step up the socioeconomic ladder corresponds with better health—not just poverty versus wealth, but fine gradations across the entire income distribution, a pattern called the social gradient in health. Countries with greater income inequality show worse population health outcomes even at similar average income levels, suggesting that relative deprivation and social hierarchy themselves harm health beyond absolute material deprivation.
Employment conditions shape health profoundly. Precarious employment—temporary contracts, part-time work without benefits, informal sector labor—associates with worse physical and mental health than stable full-time employment at similar wages, reflecting insecurity’s chronic stress. Unemployment damages health through both material deprivation and psychological harm from loss of purpose, social role, and daily structure. Hazardous working conditions in mining, agriculture, and manufacturing cause occupational diseases and injuries disproportionately affecting lower-income workers with less workplace power to demand safety improvements.
Housing quality represents a critical determinant. WHO estimates that inadequate housing contributes to approximately 100,000 deaths annually in Europe alone. Overcrowding facilitates infectious disease transmission including tuberculosis and COVID-19. Substandard housing with dampness, mold, poor ventilation, and inadequate heating causes respiratory disease, cardiovascular disease, and mental health problems. Housing instability and homelessness create cascading health harms through exposure, violence, inability to store medications or prepare nutritious food, and barriers to accessing healthcare services requiring stable addresses.
Neighborhood characteristics—sometimes called “place effects”—influence health independent of individual socioeconomic status. Residents of disadvantaged neighborhoods experience worse health than expected based on their income and education alone, reflecting neighborhood-level factors including environmental hazards (pollution, toxic waste), lack of health-promoting resources (grocery stores, parks, healthcare facilities), concentrated poverty’s psychological effects, and inadequate public services. Food deserts—areas lacking access to affordable nutritious food—force residents toward calorie-dense nutrient-poor options contributing to obesity, diabetes, and cardiovascular disease.
Gender operates as a fundamental social determinant creating health inequities distinct from biological sex differences. Discrimination, violence, unequal power in households and society, occupational segregation into lower-paying jobs, and disproportionate unpaid care burdens all harm women’s health. Yet paradoxically, women live longer than men in nearly all countries—a longevity advantage explained partly by biological factors but substantially by gender differences in health behaviors and occupational hazards, with men dying younger from violence, accidents, and chronic diseases linked to smoking, alcohol, and risky behaviors encouraged by masculine norms.
Race and ethnicity function as social determinants through discrimination, residential segregation, educational inequities, and differential exposure to environmental hazards—not biological racial differences, which WHO emphasizes are negligible. In the United States, Black Americans experience infant mortality rates 2.5 times higher than white Americans despite similar income and education levels, reflecting racism’s health impacts operating through chronic stress, differential healthcare treatment, and accumulated disadvantage across generations.
Early childhood experiences create lasting health impacts through biological embedding—the process by which social experiences literally shape developing biological systems. Children experiencing poverty, abuse, neglect, or household dysfunction show altered stress response systems, immune function, and brain development that increase lifelong disease risk. WHO estimates that investing in early childhood development could prevent 200 million children globally from failing to reach their developmental potential, with cascading effects on health across the lifespan.
Climate change operates increasingly as a social determinant, affecting health through pathways that disproportionately harm vulnerable populations: extreme heat events killing elderly and outdoor workers, flooding destroying homes and infrastructure in low-lying areas, changing disease vectors expanding malaria and dengue ranges, agricultural disruption causing malnutrition, and climate migration creating health challenges for displaced populations. Those least responsible for greenhouse gas emissions—low-income countries and disadvantaged groups within countries—bear greatest climate health burdens.
Causes, Drivers & Structural Factors
Social determinants of health don’t arise randomly or inevitably—they result from specific policy decisions, power structures, and resource allocation patterns that WHO identifies as fundamentally political rather than natural or unavoidable. According to WHO’s Commission on Social Determinants of Health, the unequal distribution of health-damaging experiences is shaped by a deeper set of structural forces including economic arrangements, social policies, and political systems that together determine how power and resources are distributed in society.
Economic systems and policies create the material conditions underlying health inequities. Macroeconomic policies prioritizing growth without attention to distribution can increase inequality even as aggregate wealth rises. Labor market deregulation, weakened unions, and erosion of worker protections shift power toward employers, enabling wage suppression, benefit reduction, and deteriorating working conditions that harm health. Trade agreements and financial liberalization can undermine domestic industries, destroy livelihoods, and reduce government revenue for health and social programs. WHO emphasizes that economic policy is health policy—choices about taxation, minimum wages, employment protections, and social safety nets directly determine population health outcomes.
Education systems stratify populations by providing unequal opportunities based on family background, geography, and ability to pay. Underfunded public schools in disadvantaged areas perpetuate intergenerational poverty through inadequate preparation for employment and higher education. Tracking systems that separate students by perceived ability often reflect and reinforce class and racial inequalities. Education financing mechanisms—particularly systems relying on local property taxes—ensure that wealthy areas have well-resourced schools while poor areas struggle with inadequate facilities, fewer experienced teachers, and limited enrichment opportunities.
Social policies determine safety net adequacy and universality. Countries with comprehensive social protection—including universal healthcare, paid parental leave, subsidized childcare, unemployment insurance, and old-age pensions—show better health outcomes and smaller health inequities than those with residual welfare systems providing minimal means-tested benefits. WHO documents that Nordic countries’ relatively egalitarian health outcomes reflect not genetic homogeneity but decades of policies ensuring high minimum income, universal services, and social solidarity.
Political systems shape who has voice and influence in decisions affecting health. Democratic governance with active civil society participation enables advocacy for health-promoting policies, while authoritarian systems or democracies with restricted participation allow powerful interests to shape policy against population health needs. Campaign finance systems permitting unlimited corporate political spending enable industries producing health-harming products (tobacco, alcohol, ultra-processed food, fossil fuels) to block regulation. Voter suppression tactics that disproportionately disenfranchise low-income and minority populations ensure their health needs receive less political attention.
Discrimination based on race, ethnicity, gender, sexual orientation, disability, and other characteristics operates as a fundamental cause of health inequities through multiple mechanisms: chronic stress from experiencing or anticipating discrimination activates physiological stress responses that damage health over time; discrimination restricts access to resources including employment, housing, credit, and education necessary for health; internalized stigma harms mental health and reduces care-seeking; and discriminatory treatment within healthcare systems results in delayed diagnosis, inadequate treatment, and medical mistrust.
Gender norms and power relations shape health through both material and psychosocial pathways. Masculine norms encouraging risk-taking, aggression, stoicism about pain and illness-seeking, and substance use contribute to men’s higher mortality from violence, accidents, and chronic diseases. Feminine norms emphasizing caregiving, self-sacrifice, and appearance create stress, constrain life choices, and enable intimate partner violence. Unequal domestic labor distribution leaves women performing the majority of unpaid care work—childcare, eldercare, housework—reducing time for health-promoting activities, education, and employment advancement.
Urbanization creates both health opportunities and risks depending on how it’s managed. Planned urbanization with investment in infrastructure, public transportation, green space, and affordable housing improves health through better access to services, employment, and social connections. Unplanned rapid urbanization produces sprawling informal settlements (slums) lacking water, sanitation, healthcare access, and safe housing—conditions where 1 billion people currently live globally. WHO emphasizes that urban health inequities often exceed rural-urban gaps, with wealthy and poor residents of the same city experiencing health outcomes differing by 10-20 years of life expectancy.
Globalization affects social determinants through complex pathways. Trade integration can increase employment and incomes in some sectors while destroying livelihoods in others. Global supply chains enable corporations to relocate production to jurisdictions with weak labor and environmental protections, exporting health hazards to countries with less regulatory capacity. International migration creates health challenges for migrants facing discrimination, dangerous transit conditions, exploitation in destination countries, and family separation, while also creating economic opportunities and remittances supporting health in origin communities.
Historical context and path dependence mean that past policies and social structures continue influencing health inequities generations later. Slavery, colonialism, indigenous dispossession, and segregation created wealth gaps, residential patterns, and institutional racism that persist despite formal legal equality. WHO’s framework recognizes that addressing health inequities requires confronting these historical injustices rather than treating current disparities as disconnected from the past.
Health Impacts Across the Lifespan
WHO identifies that social determinants affect health across the entire lifespan through cumulative mechanisms—disadvantages accumulate from conception through old age, with each life stage influenced by conditions in previous stages and shaping health in subsequent ones. This life-course perspective recognizes that adult health outcomes reflect not just current circumstances but accumulated exposures beginning before birth.
Prenatal and early childhood represent critical periods when social determinants exert disproportionate influence through biological embedding. Maternal stress, malnutrition, and exposure to environmental toxins during pregnancy alter fetal development with lasting consequences. Children born into poverty show different patterns of brain development, stress hormone regulation, and immune function compared to affluent children—differences detectable in infancy that predict health outcomes decades later. The first 1,000 days from conception to age two represent a particularly sensitive period when adequate nutrition, nurturing relationships, and safe environments are essential for optimal development.
Childhood social conditions shape educational attainment, which becomes a powerful determinant of adult health. Children from disadvantaged backgrounds enter school with developmental delays, attend under-resourced schools, face lower teacher expectations, and have less family capacity to support education—gaps that widen over years of schooling. WHO reports that educational attainment strongly predicts adult income, employment stability, health behaviors, and healthcare access, creating pathways through which childhood disadvantage translates into adult health inequities.
Adolescence represents both a vulnerable period and a window of opportunity. Adolescents from disadvantaged backgrounds face higher risks of school dropout, early pregnancy, substance use, violence, and mental health problems—all with long-term health consequences. However, interventions during adolescence—including educational support, economic opportunities, and sexual and reproductive health services—can partially compensate for early childhood disadvantage, though they cannot fully overcome it.
Working-age adults’ health reflects accumulated exposures plus current conditions. Employment quality, income stability, housing conditions, neighborhood safety, social relationships, and caregiving burdens all influence health during these peak productive years. Chronic diseases including diabetes, cardiovascular disease, cancer, and chronic respiratory disease increasingly manifest during this period, with stark social gradients—rates two to three times higher among low socioeconomic groups than high groups for most conditions.
Older adults experience health consequences of lifelong accumulation of advantage or disadvantage. Those who aged through lives of stable employment, adequate income, good housing, and social support enter old age with better physical and mental health, cognitive function, and social networks than those who experienced precarious employment, poverty, discrimination, and chronic stress. Yet social determinants continue operating in old age: pension adequacy, housing quality, social isolation, and access to age-appropriate healthcare all affect wellbeing and functional decline.
Mental health shows particularly strong social gradients across the lifespan. WHO documents that poverty, unemployment, discrimination, violence, and social isolation all increase risks of depression, anxiety, substance use disorders, and suicide. The relationship is bidirectional—mental illness can cause social and economic disadvantage, while disadvantage increases mental illness risk, creating vicious cycles difficult to escape without comprehensive support.
Chronic disease patterns reflect social determinants operating over decades. Cardiovascular disease, type 2 diabetes, chronic obstructive pulmonary disease, and many cancers show steep social gradients attributable to differential exposures to risk factors themselves socially patterned: smoking, poor diet, physical inactivity, alcohol use, and chronic stress. WHO emphasizes that framing these as “lifestyle diseases” obscures how social conditions constrain choices—poverty limits access to nutritious food and safe exercise opportunities, job stress promotes unhealthy coping mechanisms, and marketing targets disadvantaged communities with health-damaging products.
Infectious disease transmission and outcomes demonstrate social determinants’ power. COVID-19 disproportionately infected and killed disadvantaged populations through multiple pathways: inability to work from home creating workplace exposure, crowded housing facilitating household transmission, preexisting chronic conditions increasing severity, delayed care-seeking due to cost or mistrust, and lower-quality healthcare available in disadvantaged areas. This pattern—infectious diseases affecting all groups but with higher incidence and worse outcomes among disadvantaged populations—repeats for tuberculosis, HIV, hepatitis, and vaccine-preventable diseases.
Maternal and child health inequities reflect compounded social disadvantages. WHO reports that 94% of maternal deaths occur in low and middle-income countries, with further disparities within countries by income, education, urban-rural residence, and race/ethnicity. These deaths result not from medical complexity but from systematic failures to provide basic obstetric care, itself a function of social determinants: inadequate health system investment, geographic barriers to facilities, inability to afford care, and low social status of women preventing prioritization of maternal health.
Disability prevalence and impacts vary by social determinants. Disadvantaged populations experience higher disability rates through workplace injuries, inadequate prenatal care causing developmental disabilities, violence, poor management of chronic diseases, and aging without adequate support. Living with disability creates additional disadvantage through employment discrimination, inaccessible environments, and stigma—a cycle where social determinants cause disability and disability worsens social determinants.
Addressing Social Determinants: Health System and Intersectoral Responses
WHO reports that addressing social determinants requires coordinated action across multiple sectors—health, education, housing, employment, social protection, environment—because health is shaped by factors largely outside direct health sector control. According to WHO’s health in all policies framework, effective responses combine health system strengthening with intersectoral collaboration addressing root causes of health inequities.
Health system responses center on ensuring universal health coverage—access to needed health services without financial hardship—as both a social determinant itself and a mechanism for mitigating other determinants’ health impacts. WHO emphasizes that universal coverage requires: comprehensive benefit packages addressing prevention and treatment across disease areas; removal of financial barriers through tax-funded or contributory insurance systems rather than out-of-pocket payment; sufficient health workforce distributed to reach disadvantaged populations; and quality services delivered without discrimination.
Primary health care represents WHO’s preferred delivery model for addressing social determinants. Community-based primary health care approaches can identify and respond to local health needs, coordinate across sectors, address social as well as medical needs, and build community participation in health decisions. Comprehensive primary care teams including community health workers from local populations can bridge cultural and linguistic barriers, provide self-care support enabling management of chronic conditions, and link health services with social support programs.
Healthcare delivery must actively address social determinants through screening and intervention. Systematic screening for social needs—food insecurity, housing instability, intimate partner violence, social isolation—enables referral to appropriate services. Medical-legal partnerships connect healthcare with legal advocacy addressing housing, employment, benefits access, and other issues with legal dimensions. Care coordination helps patients navigate complex health and social service systems. However, WHO cautions that health sector social interventions cannot substitute for comprehensive social policies—healthcare can mitigate but not eliminate health impacts of poverty, discrimination, and disadvantage.
Education sector contributions include comprehensive sexuality education addressing sexual and reproductive health and relationships; nutrition education and school meals ensuring adequate childhood nutrition; mental health and psychosocial support addressing trauma and building resilience; and health-promoting school environments with clean water, sanitation, physical activity opportunities, and tobacco-free policies. Early childhood education programs show particularly strong health returns through cognitive development, social skills, and school readiness that translate into educational attainment and adult health.
Housing policies affect health through multiple mechanisms. Affordable housing programs prevent homelessness and housing cost burdens that force impossible choices between rent and food or healthcare. Housing quality standards requiring adequate heating, ventilation, sanitation, and safety reduce injury and disease. Mixed-income housing prevents concentrated poverty’s harms. Tenant protections limiting evictions prevent housing instability’s cascade of health harms. WHO emphasizes that treating housing as a commodity rather than a human right creates health inequities when market mechanisms allocate adequate housing to those who can pay while leaving others in substandard or unstable situations.
Employment and labor policies directly shape working-age adult health. Minimum wage policies ensuring adequate income, worker protections limiting hours and ensuring safe conditions, paid sick leave enabling illness recovery without income loss, anti-discrimination enforcement, and unionization rights enabling collective bargaining all improve health. WHO notes that while full employment and good jobs are powerful health interventions, labor market deregulation and globalization often move policy in opposite directions despite known health harms.
Social protection systems provide safety nets preventing poverty’s worst health consequences. Cash transfer programs (conditional or unconditional) improve nutrition, healthcare utilization, and child development. Unemployment insurance cushions job loss’s health impacts. Disability benefits prevent impoverishment from inability to work. Old-age pensions ensure dignified aging. Child benefits offset child-raising costs. WHO’s framework positions comprehensive social protection as essential health intervention—countries with robust systems show better population health and smaller inequities than those with minimal protections.
Environmental policies address health determinants including air and water quality, safe sanitation, toxic substance regulation, climate change mitigation and adaptation, green space preservation, and environmental justice ensuring that pollution and hazards don’t disproportionately affect disadvantaged communities. WHO reports that environmental factors cause approximately 13 million deaths annually, with burden concentrated among low-income populations in low and middle-income countries.
Urban planning and transportation policies shape health through neighborhood walkability, public transit access reducing car dependence and pollution, mixed-use development enabling proximity to daily needs, parks and recreational facilities supporting physical activity, and affordable housing integrated into neighborhoods with employment and services. Car-dependent sprawl worsens health through air pollution, traffic injuries, physical inactivity, and social isolation, while compact walkable urban design promotes health.
Criminal justice reform addresses health harms from mass incarceration, which disproportionately affects low-income and minority communities. Incarceration disrupts families, traumatizes children, concentrates infectious disease, causes mental health deterioration, and creates barriers to employment and housing after release. Alternatives including community-based treatment for substance use and mental illness, restorative justice programs, and decriminalization of survival behaviors (sex work, drug use) reduce these harms. Police violence represents a direct health threat in communities experiencing aggressive enforcement.
Prevention Through Structural Change and Policy Interventions
WHO’s prevention framework for social determinants emphasizes upstream interventions addressing root causes rather than downstream responses treating consequences. According to WHO’s equity action framework, effective prevention requires tackling the fundamental distribution of power, money, and resources that create health-harming social conditions, alongside targeted interventions for populations experiencing greatest disadvantage.
Redistributive economic policies reduce income and wealth inequality that drives health inequities. Progressive taxation where higher earners pay proportionally more revenue can fund universal services and social programs. Minimum wage policies ensure adequate income from full-time work. Maximum wage ratios limit extreme compensation disparities. Capital gains taxation reduces wealth concentration. Estate taxes prevent perpetuation of dynastic wealth. Universal basic income pilots show health benefits through income security and stress reduction, though scalability and sustainability remain debated.
Early childhood investment represents perhaps the most cost-effective social determinant intervention. WHO cites evidence that comprehensive programs including: prenatal care and support, paid parental leave enabling caregiving, home visiting for high-risk families, high-quality affordable childcare and preschool, child nutrition programs, and developmental screening with early intervention—produce returns exceeding $7 for every dollar invested through improved health, education, employment, and reduced social costs across lifespans.
Educational equity policies aim to equalize opportunities regardless of family background. Universal free public education from preschool through higher education removes financial barriers. Equitable school funding based on student needs rather than local property wealth addresses resource gaps. Integrated schools (by income, race) reduce concentrated poverty’s harms. Universal school meals ensure nutrition. Affirmative action in higher education partially compensates for cumulative disadvantage. However, WHO notes that educational interventions alone cannot overcome health inequities rooted in material conditions—educated people living in poverty still experience poverty’s health harms.
Universal health coverage represents both an intervention addressing a social determinant (healthcare access) and a broader equity strategy. WHO’s framework emphasizes that achieving universal coverage requires political commitment to health as a human right, progressive financing preventing financial hardship from healthcare costs, and delivery systems reaching disadvantaged populations. Countries achieving universal coverage through single-payer systems, social health insurance, or other mechanisms show smaller health inequities than those relying on market-based systems or means-tested programs.
Labor market interventions address employment’s health impacts. Policies include: living wage requirements, worker protections limiting hours and ensuring rest, occupational health and safety enforcement, paid family and medical leave, unemployment insurance, portable benefits for gig workers, union rights enabling collective bargaining, and anti-discrimination enforcement. WHO emphasizes that full employment at decent wages represents a powerful health intervention, requiring macroeconomic policies prioritizing employment alongside price stability.
Housing policies ensuring adequate affordable housing for all include: social housing programs providing public alternatives to private markets, rent control and tenant protections preventing displacement, housing-first approaches for homelessness, mixed-income development requirements in new construction, inclusionary zoning mandating affordable units, and housing quality enforcement. Countries treating housing as a human right through constitutional provisions show smaller housing-related health inequities than those treating it purely as a commodity.
Anti-discrimination law and enforcement reduce health harms from racism, sexism, homophobia, and other forms of systematic disadvantage. Comprehensive civil rights protections covering employment, housing, education, and services; enforcement mechanisms with real penalties; and affirmative measures addressing historical discrimination all contribute. However, WHO cautions that legal equality doesn’t automatically produce health equity—power differentials and structural racism persist despite formal protections.
Environmental justice policies prevent disproportionate exposure of disadvantaged communities to pollution and hazards. Siting regulations preventing concentration of polluting facilities in low-income neighborhoods, environmental impact assessments considering equity effects, community right-to-know about local hazards, and polluter-pays principles funding cleanup all contribute. Climate adaptation policies must prioritize vulnerable populations experiencing greatest climate health impacts.
Participatory governance enables affected communities to shape policies impacting their health. Mechanisms include: community representation in decision-making bodies, participatory budgeting allocating public resources, community-based participatory research engaging communities in defining health priorities and research questions, and social movements advocating for health equity. WHO emphasizes that communities experiencing health inequities must have power in defining problems and solutions—expert-driven approaches often miss key issues or propose solutions that don’t fit local contexts.
WHO’s Global Efforts and the Commission on Social Determinants of Health
WHO’s Commission on Social Determinants of Health, established in 2005 and reporting in 2008, marked a watershed in global recognition that health inequities result from modifiable social conditions rather than inevitable biology or geography. The Commission’s final report, “Closing the Gap in a Generation,” documented that social injustice kills on a massive scale and proposed comprehensive actions across society to achieve health equity within a generation. According to WHO’s Commission report, three overarching recommendations guide action: improve daily living conditions, tackle inequitable distribution of power and resources, and measure and understand the problem.
The Commission’s legacy includes establishing social determinants as central to global health discourse, influencing national health policies in over 60 countries that developed action plans addressing social determinants, and creating frameworks for intersectoral collaboration on health. However, critics note that implementation has been uneven—while rhetoric embracing social determinants is widespread, political and economic interests often block the structural changes required to reduce health inequities.
WHO’s Health in All Policies approach, refined since 2010, operationalizes social determinant action by systematically considering health impacts of decisions across government sectors. The framework guides policy-makers in: assessing health equity impacts of proposed policies, strengthening accountability for health impacts across sectors, building intersectoral collaboration mechanisms, and engaging stakeholders including affected communities. Countries implementing health in all policies—notably Finland, Thailand, and South Australia—report successes in policy coordination, though measuring population health impacts remains challenging given long time lags between policy changes and health outcomes.
The Rio Political Declaration on Social Determinants of Health, adopted at WHO’s 2011 World Conference, committed governments to action on social determinants through five strategic areas: adopt better governance for health and development, promote participation in policy-making and implementation, reorient the health sector toward reducing health inequities, strengthen global governance and collaboration, and monitor progress. The declaration represented political acknowledgment at the highest levels that social determinants require action, though subsequent progress has been limited by competing priorities, economic constraints, and political opposition to redistributive policies.
WHO’s Commission on the Social Determinants of Health established in 2023—distinct from the original 2005-2008 Commission—reflects recognition that the problem remains urgent. This new Commission addresses emerging challenges including: COVID-19’s exacerbation of health inequities, climate change’s differential health impacts, digital technology’s role in creating or reducing inequities, and commercial determinants of health (corporate practices harming health). The Commission’s interim reports highlight concerning trends: health inequities widening within many countries despite overall health improvements, and political commitment to equity weakening in some regions as nationalism and xenophobia increase.
Regional WHO offices develop context-specific approaches to social determinants. The Pan American Health Organization pioneered equity-focused strategic plans addressing racism, poverty, and gender as health determinants in the Americas. WHO’s European Region emphasizes healthy cities initiatives integrating health into urban planning. The African Region focuses on governance, education, and infrastructure as foundations for health equity. The South-East Asia Region addresses caste, tribal status, and gender as structural determinants. The Western Pacific Region examines rapid urbanization and economic transition’s health equity implications.
WHO’s partnership strategy engages diverse actors beyond health ministries. The organization collaborates with: UN agencies including UNICEF (child welfare), ILO (labor conditions), UN-Habitat (urban planning), and UNDP (development); the World Bank on health and development financing; civil society organizations advocating for disadvantaged populations; academic institutions researching social determinants; and increasingly, partnerships examining commercial determinants where corporate practices harm health.
The Sustainable Development Goals (SDGs), adopted in 2015, embed social determinants throughout the framework. While SDG 3 directly addresses health, determinants appear in goals addressing poverty (SDG 1), hunger (SDG 2), education (SDG 4), gender equality (SDG 5), clean water and sanitation (SDG 6), decent work (SDG 8), reduced inequalities (SDG 10), sustainable cities (SDG 11), climate action (SDG 13), and partnerships (SDG 17). WHO emphasizes that achieving health goals requires progress across all SDGs—health cannot be separated from broader development.
Monitoring and accountability mechanisms track progress on social determinants and health equity. WHO’s Health Equity Monitor enables countries to track inequities in health outcomes and service access by wealth, education, residence, and other stratifiers. The organization’s annual World Health Statistics reports increasingly disaggregate data to reveal within-country inequities. However, data gaps remain severe, particularly for marginalized populations including migrants, indigenous peoples, and stigmatized groups who may be invisible in standard surveillance systems.
Contemporary challenges complicate social determinant action. The COVID-19 pandemic devastated progress on multiple fronts: increasing poverty through economic disruption, widening educational gaps through school closures affecting disadvantaged students most severely, exacerbating mental health problems through isolation and stress, and revealing brutal health inequities in infection, severity, and economic impacts. Recovery efforts now grapple with how to build back better rather than returning to pre-pandemic inequities.
Climate change operates increasingly as a fundamental determinant requiring systemic responses. WHO’s framework positions climate action as health action, with mitigation preventing future health harms and adaptation protecting vulnerable populations from current impacts. Just transition policies ensuring that climate action doesn’t worsen inequities—for example, supporting fossil fuel workers’ transition to green industries rather than abandoning them—represent critical equity considerations.
Digital health equity has emerged as a key concern. While digital health technologies promise improved access and quality, they risk widening inequities if benefits accrue primarily to affluent populations with internet access, digital literacy, and appropriate devices while disadvantaged populations are left behind. WHO’s guidance emphasizes designing digital health interventions to reduce rather than reinforce existing inequities.
Commercial determinants of health—corporate practices and power harming health—receive increasing WHO attention. Industries producing health-damaging products (tobacco, alcohol, ultra-processed food, fossil fuels) actively oppose regulation while marketing aggressively to disadvantaged populations. Corporate lobbying, campaign financing, industry-funded research, and revolving door personnel moves between industry and regulation undermine public health policies. WHO’s framework positions commercial determinants as structural drivers requiring political action to constrain corporate power and prioritize health over profits.
Understanding social determinants connects to contemporary challenges including refugee and migrant health where vulnerable people on the move experience compounded disadvantages; sexual health inequities reflecting gender, income, and discrimination; and the need for accessible care extending to all populations including those with disabilities as highlighted through accessibility awareness initiatives. These specific issues illustrate broader patterns where social position determines health outcomes.
The fundamental challenge remains political: implementing policies addressing social determinants requires confronting powerful interests benefiting from current inequitable arrangements. Redistributive policies face opposition from those currently advantaged. Corporate regulation encounters massive industry resistance. Rights-based approaches challenge those comfortable with hierarchy. WHO can document evidence, provide technical guidance, and advocate for equity—but cannot compel member states to adopt policies that their political systems resist. This tension between technical knowledge and political feasibility means that despite decades of evidence that social determinants are the primary drivers of health outcomes, health policy still focuses disproportionately on medical interventions addressing symptoms rather than root causes.
Historical patterns visible across world history show that major reductions in health inequities have typically required social movements, political upheaval, or crises forcing fundamental restructuring—postwar social democratic settlements in Europe, civil rights movements in the US, independence movements ending colonialism. Whether contemporary societies will choose to address health inequities through deliberate policy or will require similar upheavals remains an open question that WHO’s social determinants framework cannot answer—only illuminate.
Frequently Asked Questions
WHO identifies key social determinants as: income and social status, education, employment and working conditions, social support networks, physical environments, personal health practices and coping skills, healthy child development, biology and genetics, health services, gender, and culture. These determinants interact and cluster—poverty affects housing, education, employment, and nutrition simultaneously. WHO emphasizes that these conditions are shaped by the distribution of money, power, and resources at global, national, and local levels through policy choices.
According to WHO, health systems account for only 10-20% of health outcomes, while social determinants including education, income, employment, and environment drive 80-90%. Genetics explain a small proportion of population-level health differences—the 18-year life expectancy gap between low and high-income countries isn’t genetic but reflects social conditions. People with identical genetic backgrounds show dramatically different health outcomes based on socioeconomic position, demonstrating that social circumstances outweigh biology in determining population health patterns.
WHO reports that while individual behaviors matter, they’re largely shaped by social conditions rather than purely personal choices. Poverty limits access to nutritious food and safe exercise opportunities; job stress promotes unhealthy coping mechanisms; marketing targets disadvantaged communities with health-damaging products. Data show that even when controlling for health behaviors, social gradients in health persist—wealthy smokers live longer than poor non-smokers in many populations. Individual behavior change cannot overcome systematic differences in living and working conditions.
According to WHO, countries with smaller health inequities typically have: comprehensive social protection systems including universal healthcare; progressive taxation funding public services; strong labor protections ensuring decent employment; investments in education and early childhood; affordable housing policies; and political systems enabling broad participation in decisions affecting health. Nordic countries exemplify this pattern. Countries with minimal social protection, weak labor rights, and high inequality show larger health gaps despite sometimes having higher average wealth.
WHO identifies health system actions including: screening for social needs and linking to services, medical-legal partnerships addressing housing and employment issues, community health workers providing culturally appropriate care, care coordination navigating complex systems, and advocacy for policies addressing root causes. However, WHO emphasizes that health systems alone cannot eliminate health impacts of poverty, discrimination, and disadvantage—they can mitigate but not substitute for comprehensive social policies addressing distribution of power and resources.
Sources
- World Health Organization. Social Determinants of Health. https://www.who.int/health-topics/social-determinants-of-health
- Commission on Social Determinants of Health. Closing the gap in a generation: health equity through action on the social determinants of health. Geneva: World Health Organization; 2008. https://www.who.int/publications/i/item/WHO-IER-CSDH-08.1
- World Health Organization. Health in All Policies: Helsinki Statement. Geneva: World Health Organization; 2013. https://www.who.int/publications/i/item/9789241563970
- Marmot M, et al. Health equity in England: The Marmot Review 10 years on. BMJ. 2020;368:m693.
Disclaimer
This article adapts publicly available information from WHO’s Social Determinants of Health page. This content is for informational and educational purposes only and does not constitute medical advice. ObserverVoice.com is a news and information platform—not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.