
Gout: Why Uric Acid Crystals Form in Joints and What Triggers an Attack
Imagine a middle-aged man awakening at 3 AM with excruciating pain in his big toe. The joint is swollen, red, warm. Exquisitely tender. Any touch causes severe pain. Walking impossible. He cannot bear weight on the foot. The pain is described as the worst he has ever experienced. Fever present. Malaise. Within hours, he arrives at the emergency department. X-rays normal. Blood work reveals elevated uric acid at 8.5 mg/dL (normal less than 6.8). Synovial fluid aspiration reveals needle-shaped crystals under microscopy—monosodium urate. Diagnosis: acute gout attack. Colchicine, NSAIDs, and glucocorticoids prescribed. Within 48 to 72 hours, pain subsides. Inflammation resolves. Yet without understanding gout’s cause and implementing prevention, attacks recur monthly. Years of recurrent attacks. Multiple affected joints. Chronic tophaceous gout. Permanent joint damage. Yet prevention is possible. Uric acid-lowering medication. Dietary modification. Hydration. Weight management. These simple interventions prevent attacks and preserve joint function. Understanding gout enables appropriate treatment and prevention preventing recurrent debilitating attacks and permanent joint damage. Gout is a form of crystal arthritis caused by monosodium urate crystal deposition in joints, triggering acute inflammatory attacks. Gout affects approximately 1 to 3 percent of the population. Approximately 8 to 10 million Americans have gout. Gout is the most common inflammatory arthritis in men. The prevalence is increasing globally due to increased purine intake in modern diets and increased prevalence of obesity, hypertension, and chronic kidney disease. What makes gout important is understanding that while acute attacks are extremely painful, gout is largely preventable through lifestyle modification and medication. Early recognition and appropriate treatment prevent recurrent attacks and permanent joint damage. Understanding gout enables appropriate acute and chronic management preventing disability and improving quality of life. In this comprehensive article, we will explore what gout is, understand uric acid metabolism and crystal formation, recognize symptoms of gout attacks, explore risk factors and triggers, and discover prevention and treatment strategies.
Understanding Uric Acid Metabolism and Crystal Formation
Before we explore gout, we need to understand uric acid metabolism and how crystals form in joints. Purine metabolism. Purines. Nitrogenous bases. DNA. RNA. Adenine. Guanine. Nucleotides. Nucleic acids. Components. Dietary sources. Meat. Seafood. Organ meats. Yeast. Beer. High-purine foods. Purine-rich. Endogenous synthesis. Cells. Nucleotide synthesis. DNA. RNA. Purine metabolism breakdown. Adenosine. Inosine. Hypoxanthine. Xanthine. Uric acid. Sequential. Enzymatic. Degradation. Xanthine oxidase. Final enzyme. Xanthine converted. Uric acid. Final product. Human purine metabolism. Uric acid. End product. Cannot further metabolized. Humans. Unlike other mammals. Uricase enzyme. Absent. Lost during evolution. Primates. Humans. Uric acid. Circulates. Blood. Kidney filtered. Urine excreted. Serum uric acid. Concentration. Approximately 3.5 to 7.2 mg/dL. Men. Approximately 2.6 to 6.0 mg/dL. Women. Gender difference. Estrogen. Uric acid. Renal excretion. Enhances. Women. Lower levels. Premenopausal. Postmenopausal. Levels increase. Estrogen loss. Excretion. Reduced. Uric acid saturation. Serum. 6.8 mg/dL. Saturability point. Approximately. Temperature. Dependent. Cooler. Peripheral joints. Solubility. Reduced. Crystal formation. More likely. Monosodium urate crystal formation. Serum uric acid. Supersaturation. Occurs. Approximately 6.8 mg/dL. Above. Crystals precipitate. Monosodium urate. Needle-shaped. Rhomboid. Crystal structure. Formation. Nucleation. Induction. Precipitation. Protein. Crystals. Proteoglycans. Lipoproteins. Lower levels. Support. Joint fluid. Uric acid concentration. Higher. Serum. 30 to 50 percent higher. Joint space. Synovial fluid. Supersaturation. More likely. Peripheral joints. Toes. Ankles. Knees. Risk. Temperature. Cooler periphery. Solubility. Lower. Crystal precipitation. Facilitated. Factors promoting crystal formation. Hyperuricemia. Elevated serum uric acid. Above 6.8 mg/dL. Risk. Crystal formation increased. Causes hyperuricemia. Increased production. Purine-rich diet. High-fructose. Alcohol especially beer. Cell turnover. Leukemia. Hemolysis. Chemotherapy. Tumor lysis syndrome. Reduced excretion. Chronic kidney disease (CKD). Reduced kidney. Uric acid filtration. GFR declining. Uric acid accumulates. Medications. Diuretics. Loop thiazide. Uric acid. Reabsorption. Increases. Excretion. Reduced. Aspirin. Low-dose. Uric acid reabsorption. Increases. High-dose. Uric acid excretion. Increases. Lesch-Nyhan syndrome. Rare genetic. HGPRT enzyme. Deficiency. Purine metabolism. Dysregulation. Massive uric acid overproduction. Acidosis. Metabolic. Lactic acidosis. Ketoacidosis. Uric acid. Renal tubular reabsorption. Increased. Acidosis. Associated. Uric acid concentration. Local joint. Dehydration. Serum uric acid. Concentration. Increases. Crystal formation. Risk. Increased. Trauma. Joint. Mechanical stress. Crystal nucleation. Trigger. Cooling. Joint temperature. Reduced. Solubility lower. Crystal precipitation. Favored. Gout attacks. Often. Night. Early morning. Cooler body temperatures. Associated. Joint trauma. Sometimes triggers. Acute attack. Alcohol consumption. Ethanol. Uric acid production. Increases. Excretion. Reduces. Hyperuricemia worsens. Acute attack. Possible. Beer. Particularly. High guanosine content. Additional purine source. Purines. Metabolism. More uric acid produced. Fructose. High fructose consumption. Fructose metabolism. ATP depletion. Adenosine. Adenine increased. Purine metabolism. Amplified. Uric acid production. Enhanced. High-fructose corn syrup. Sugary beverages. Processed foods. High-fructose. Associated. Gout. Risk. Escalation. The pathophysiology explains why hyperuricemia and crystal deposition cause inflammatory arthritis.
What is Gout?
Gout is a form of crystal arthritis caused by monosodium urate crystal deposition in joints and surrounding tissues, triggering acute inflammatory attacks. Classification. Acute gouty arthritis. Acute attack. Sudden onset. Severe. Inflammation. Monosodium urate crystals. Synovial fluid. Acute attack characteristics. Severe pain. Joint. Sudden onset. Reaches peak. Hours. Swelling. Redness. Warmth. Overlying skin. Erythema. Fever. Possible. Joint movement. Severely limited. Exquisite tenderness. Any touch. Extreme pain. Duration. Days to weeks. Untreated. Resolving. Gradual. Anti-inflammatory medication. Treatment. Days. Usually resolves. Intercritical period. Period between attacks. Asymptomatic. Usually. No joint symptoms. Serum uric acid. Usually elevated. Persistent. Chronic tophaceous gout. Recurrent attacks. Chronic hyperuricemia. Urate deposits. Tophi. Hard masses. Cartilage. Subcutaneous tissue. Ears. Fingers. Elbows. Feet. Visible. Cosmetic. Palpable nodules. Joint damage. Chronic tophaceous gout. Permanent. Joint destruction. Erosions. Bone. Cartilage. Deformity. Loss of function. Asymptomatic hyperuricemia. Elevated serum uric acid. No gout attacks. Asymptomatic. Approximately 85 percent. Hyperuricemia population. Never develop gout. Asymptomatic. Screening. Serum uric acid. Discovery. May be incidental. No treatment. Indicated. Progression. Some. Gout attacks. Develop. Years. Decades later. Prevalence. Gout. Approximately 1 to 3 percent. Population. Approximately 8 to 10 million Americans. Male predominance. Approximately 4:1 ratio. Men to women. Menopause. Women. Incidence. Increases. Estrogen. Uric acid excretion. Decreases. Age. Older. Prevalence higher. Men. Peak incidence. Age 40 to 60 years. Women. Peak incidence. Age 60 to 70 years. Post-menopausal. Ethnicity. Higher prevalence. Pacific Islanders. Maori. Aboriginal Australians. Genetic predisposition. Important. Familial clustering. Common. Approximately 60 percent. Gout patients. Family history. Multiple genes. Involved. Urate transporters. Kidney. Genes affecting. URAT1. GLUT9. Others. Uric acid reabsorption. Genetic variation. Individual susceptibility. Uric acid levels. Gout. Complex inheritance. Multi-factorial. The clinical features vary widely from asymptomatic hyperuricemia to disabling chronic tophaceous gout.
Recognizing Gout: Acute Attacks and Clinical Presentation
Gout has distinctive presentations recognizable by sudden onset of severe joint pain and characteristic examination findings. First gout attack (typically age 40-60). Sudden onset. Middle of night. Early morning. Awakening. Severe pain. Joint. Big toe. Most common. Approximately 50 percent. First attack. Podagra. Foot involvement. Ankle. Knee. Wrist. Other joints. Possible. But less common. Pain severity. Excruciating. Described. Worst pain. Ever experienced. Severe. Mobility. Severely restricted. Walking. Impossible. Touching joint. Exquisite. Tenderness. Unbearable. Swelling. Rapid onset. Hours. Foot. Markedly swollen. Redness. Overlying skin. Erythema. Bright red. Intense. Appearance. Resembles infection. Cellulitis. Sometimes mistaken. Skin. Shiny. Appearance. Warmth. Joint. Warm to touch. Fever. Sometimes present. Malaise. Chills. Constitutional symptoms. Possible. Severe attack. Acute. Urgent. Many. Seek emergency care. Misdiagnosis. Cellulitis. Infection. Sometimes initial. Antibiotics started. Ineffective. Gout. Recognized. Later. Subsequent attacks. Recurrent. Pattern. Variable. Some. Attack. One year. Others. Multiple. Year. Frequency. Unpredictable. Usually. Without uric acid-lowering medication. Increased. Escalates. Years. Attack interval. Shortens. Severity. Increases. Additional joints affected. Chronic gout. Progressive. Asymptomatic hyperuricemia (any age). Elevated uric acid. Discovered. Screening labs. Asymptomatic. No symptoms. Joint pain. No swelling. No attacks. Incidental finding. Uric acid. Greater than 6.8 mg/dL. Sometimes. Years. No progression. Gout never. Asymptomatic. Indefinite. Other times. Gout attacks. Eventual. Development. Years. Decades. Later. Risk factors. Present. Obesity. Hypertension. Diuretic use. Chronic kidney disease. Dietary factors. Alcohol. Purine. Fructose. Risk. Escalation. Attacks. Development. Likely. Prevention. Emphasized. Intercritical gout (between attacks). Asymptomatic. Period. Between attacks. Serum uric acid. Usually elevated. Persistent. Above 6.8. Target below 6 mg/dL. Urate-lowering therapy. Intended. If treatment. Persistent elevation. Uric acid. Crystal formation. Continued. Risk. New attacks. Joint damage. Progressive. Prevention. Uric acid-lowering medication. Critical. Chronic tophaceous gout (late stage). Recurrent. Uncontrolled. Attacks. Chronic hyperuricemia. Years. Urate deposits. Tophi. Develop. Fingers. Ears. Elbows. Feet. Subcutaneous. Hard nodules. Multiple. Visible. Cosmetic concern. Hands. Deformity. Visible. Social. Psychological impact. Significant. Joint damage. Progressive. Chronic. Erosions. Cartilage. Bone. Joint space. Narrowing. Deformity. Secondary osteoarthritis-like changes. Joint function. Loss. Permanent. Surgical intervention. Sometimes. Tophi removal. Or joint replacement. Severe damage. Triggering factors. Recognition. Important. Common triggers. Alcohol consumption. Particularly beer. Single episode. Alcohol. Gout attack. Triggered. 24 to 48 hours. Post-consumption. Purine-rich foods. Large meal. Meat. Seafood. Organ meats. High purine. Gout attack. Possible. Hours. Following meal. Dehydration. Inadequate fluid intake. Uric acid concentration. Blood. Increases. Crystal formation. Encouraged. Strenuous exercise. Intense. Physical exertion. Dehydration. Associated. Uric acid. Elevation. Gout triggered. Joint trauma. Minor injury. Joint. Mechanical stress. Crystal nucleation. Trigger. Acute attack. Surgery. Medical illness. Acute illness. Stress. Fever. Metabolism. Altered. Uric acid. Elevated. Acute attack. Triggered. Medications. Initiation. Diuretics. Aspirin. Uric acid-lowering agents. Initially. Paradoxically. Uric acid manipulation. Attacks. Trigger. Mechanism. Complex. Adjustment. Joints. Urate load. Altered. Crystal mobilization. Attacks. Possible. First weeks. Uric acid-lowering therapy. The diverse presentations and triggers require comprehensive understanding for appropriate management.
Diagnosis: Joint Fluid Analysis and Uric Acid Testing
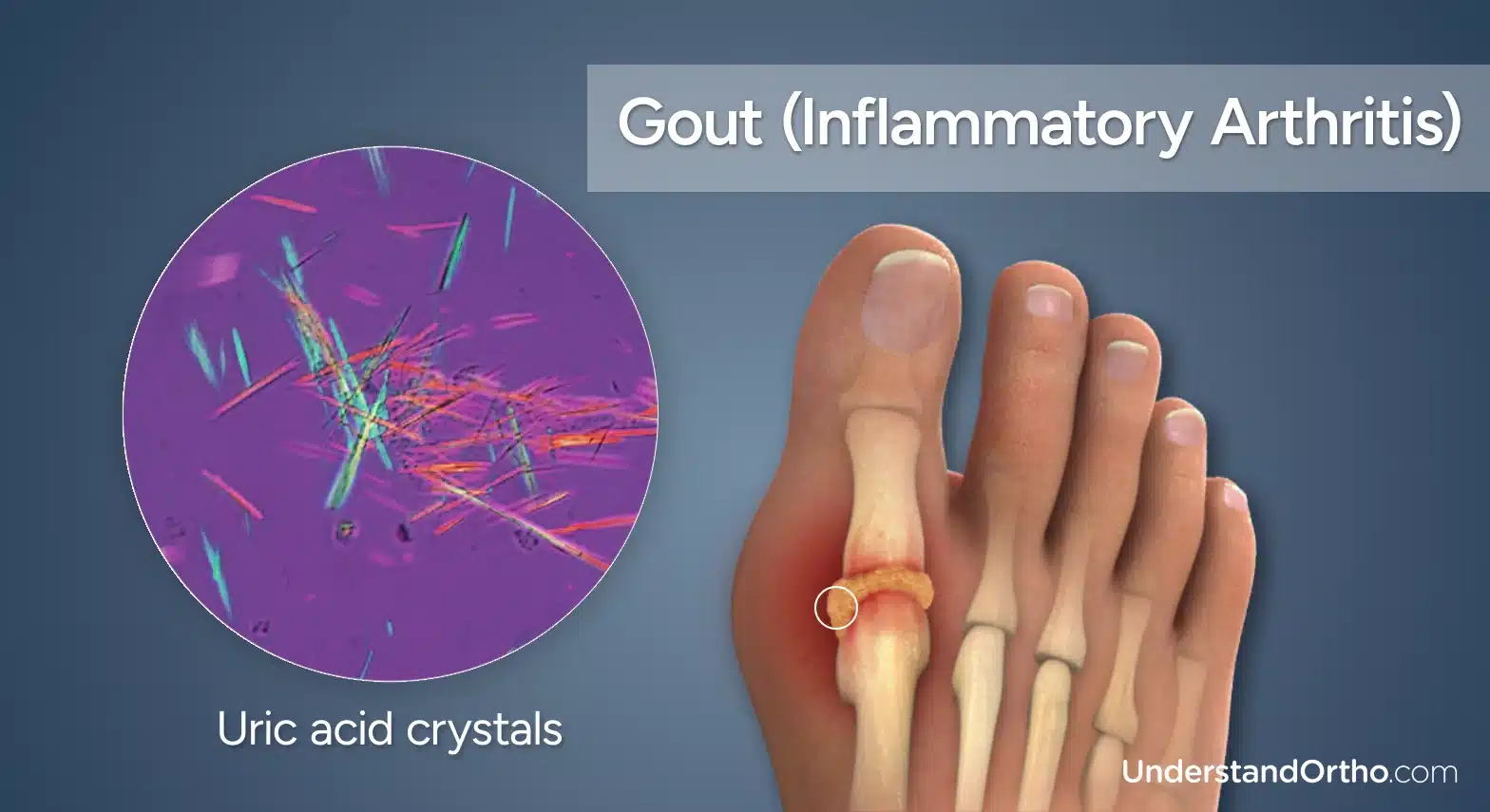
Diagnosing gout requires demonstration of monosodium urate crystals in synovial fluid obtained by arthrocentesis. Clinical suspicion. History. First attack. Sudden onset. Severe pain. Nocturnal. Foot involvement. Most common. Risk factors. Obesity. Hypertension. Chronic kidney disease. Alcohol. Purine diet. Clinical examination. Joint. Swollen. Red. Warm. Tender. Movement. Severely limited. Fever possible. Malaise. Constitutional symptoms. Acute. Appearance. Resembles infection. Cellulitis differential. Important. Synovial fluid analysis. Arthrocentesis. Aspiration. Joint fluid. Examination. Crystal identification. Definitive. Gold standard. Diagnosis. Monosodium urate crystals. Needle-shaped. Negatively birefringent. Polarized microscopy. Characteristic. Under polarized light. Crystals. Appear. Blue. Parallel to microscope compensator. Negative birefringence. Specific for monosodium urate. Differentiates. Calcium pyrophosphate. Pseudogout. Crystals. Positively birefringent. Rhomboid-shaped. Different from gout. White blood cells. Synovial fluid. Elevated. Acute gout. Typically 5,000 to 75,000 cells/μL. Range variable. Majority. Neutrophils. Predominance. Infection. Rules out. Negative culture. Bacteria. Absent. Usually. Some overlap. Infection. Crystal arthritis. Coexistence. Possible. Gram stain. Culture. Blood cultures if infection suspected. Complete differential. Fluid analysis. Glucose. Protein. Characteristics. Crystals present. Gout. Likely diagnostic. Serum uric acid. Tested. Baseline. Often elevated. Greater than 6.8 mg/dL. Acute attack. Sometimes normal. Attack resolution. Rapid. Uric acid may normalize. Testing. Attack. May not capture elevation. Uric acid. Weeks. Post-attack. Testing. Recommended. Baseline. Chronically elevated. Uric acid. Approximately 90 percent. Gout patients. Documented. Normal uric acid. Gout attack. Does not exclude. Approximately 5 to 10 percent. Gout patients. Normal serum uric acid. Possible mechanism. Variation. Individual. Kidney handling. Serum-synovial. Gradient. Concentrated. Joint. Lower serum. Crystals. Form. Joint. Serum. Normal. X-rays. Imaging. Early gout. X-rays normal. Useful rule out. Other pathology. Fracture. Infection. Bone abnormality. Chronic gout. Erosions visible. Characteristic appearance. Overhanging edge. Bone erosion. Cortex. Overhanging. Soft tissue. Tophi. Visible. Calcified. Dense. Imaging findings. Chronic. Supportive diagnosis. Ultrasound. Monosodium urate crystals. Detected. Double contour sign. Hyperechoic line. Cartilage surface. Characteristic. Crystal deposition. Specific for gout. Not routine. Research. Emerging. CT or MRI. Advanced imaging. Complex cases. Severe chronic tophaceous gout. Deformity. Severity assessment. Surgical planning. The diagnosis requires synovial fluid analysis with crystal identification under polarized microscopy as the gold standard.
Management: Acute Attack Treatment and Long-Term Prevention
Gout management requires treatment of acute attacks and chronic uric acid-lowering therapy to prevent recurrence. Acute attack management. Anti-inflammatory medications. NSAIDs (nonsteroidal anti-inflammatory drugs). First-line. Indomethacin. Naproxen. Ibuprofen. Dose. High initially. Pain control. Rapid. Taper. Days to weeks. Colchicine. Traditional. Low-dose. 0.6 mg twice daily. Hours. Acute attack. Effective. GI side effects. Diarrhea. Nausea. Common. Limits tolerability. High-dose colchicine. Previously used. More GI toxicity. Low-dose. Current standard. Glucocorticoids. Oral. Prednisone. Prednisolone. 30 to 40 mg daily. Days. Taper. Over 1 to 2 weeks. Effective. Particularly. NSAIDs contraindicated. Renal disease. Heart failure. GI ulcers. Intra-articular injections. Glucocorticoid. Joint directly. Excellent response. Rapidly. Particularly. Single joint. Affected. Polyarticular gout. Systemic therapy. Preferred. Rest. Ice. Elevation. Joint. Supportive measures. Pain management. Reduces. Combined. Medications. Optimal. Hydration. Fluid intake increased. Uric acid concentration. Blood. Dilutes. Excretion. Enhanced. Urine output. Increased. Crystal precipitation. Reduced. Pain management. Opioids. Sometimes. Short-term. Severe pain. Refractory. NSAIDs. Colchicine. Glucocorticoids. Inadequate. Morphine. Other opioids. Options. Addiction risk. Dependence. Concerns. Short-term. Acceptable. Acute attack. Chronic management. Uric acid-lowering therapy. Target. Serum uric acid. Less than 6 mg/dL. Approximately. Below saturation point. Crystal dissolution. Promotes. Xanthine oxidase inhibitors. Allopurinol. First-line. Long-term. Uric acid-lowering therapy. Blocks. Xanthine oxidase. Final enzyme. Purine metabolism. Uric acid production. Reduced. Approximately 75 to 90 percent. Uric acid reduction. 300 mg daily. Starting dose. Titration. Gradual. Up to. 800 mg daily. Sometimes higher. Target. Serum uric acid. Less than 6 mg/dL. Achievement. Weeks to months. Monitoring. Important. Dose adjustment. Renal function. Important. eGFR less than 30. Dose reduction. Necessary. Allopurinol hypersensitivity syndrome. Rare. Severe. Rash. Fever. Hepatitis. Kidney dysfunction. Life-threatening. If suspect. Discontinue immediately. Alternative agents. Febuxostat. Xanthine oxidase inhibitor. Selective. More potent. 40 to 80 mg daily. Similar efficacy. Allopurinol. More expensive. Alternative. Allopurinol intolerance. Allergy. Uricosuric agents. Probenecid. Increases. Uric acid excretion. Kidney. Urine. Urinary uric acid loss. Increases. Serum uric acid. Falls. 500 to 3000 mg daily. Dosing. Variable. Uric acid. Increased urine. Stone formation. Risk. High urinary uric acid. Fluid intake. Important. Urate oxidase. Pegloticase. Enzyme. Uric acid. Converted. Allantoin. Non-toxic. Readily excreted. Particularly effective. Severe. Chronic tophaceous gout. Refractory. Allopurinol. Febuxostat. Others. IV administration. Twice monthly. Dramatically. Serum uric acid. Reduction. Cost. Extremely high. Reserved. Severe refractory. Gout. Attack prophylaxis. Uric acid-lowering therapy. Started. Attacks. Initially. Triggered. Medications. Colchicine. Low-dose. Prophylaxis. 0.6 mg daily. Weeks to months. Uric acid-lowering therapy. Initiated. Protective. Reduces. Attack frequency. NSAIDs prophylaxis. Low-dose indomethacin. Naproxen. Alternatives. Glucocorticoids. Low-dose. Prophylaxis. Prednisone. 5 to 10 mg daily. Options. Duration. Prophylaxis. Approximately 3 to 6 months. Therapy initiation. Continuing. If attacks occur. Taper discontinuation. Gradually. Abrupt cessation. Attacks. Triggered. Slow tapering. Important. Lifestyle modifications. Weight loss. 5 to 10 percent. Weight reduction. Uric acid. Decreases. Gout. Risk reduction. Exercise. Regular. Cardiovascular. Beneficial. Weight management. Important. Diet modifications. Purine reduction. Meat. Seafood. Organ meats. Limited. High-purine foods. Reduced. Fish. Fish oil. Omega-3. Some benefit. Red meat. More associated. Gout than poultry. Poultry. Lower risk. Dairy. Protective. Low-fat dairy. Especially beneficial. Alcohol. Elimination. Or substantial reduction. Beer. Particularly. High guanosine. Liquor. Wine. Less associated. Gout than beer. Fructose. High-fructose corn syrup. Sugary beverages. Limited. Fructose metabolism. Uric acid. Increases. Hydration. Adequate. Fluid intake. 2 to 3 liters daily. Urine output. Increased. Uric acid excretion. Enhanced. Uric acid. Dilution. Crystal formation. Risk. Reduced. Medications review. Diuretics. Loop. Thiazide. Uric acid. Elevation. Alternative. ACE inhibitor. ARB. Better choice. Hypertension. Gout. Both. Aspirin. Low-dose. Uric acid reabsorption. Increased. Avoided if possible. High-dose. Uric acid excretion. Increased. Preferred. But rarely used. Modifying risk factors. Management. Hypertension. Blood pressure control. Obesity. Weight loss. Chronic kidney disease. GFR monitoring. Management. Progressive. CKD. Uric acid levels. Elevation. Metabolic syndrome. Components. Management. Important. The comprehensive approach addresses acute attacks and chronic prevention preventing recurrent debilitating attacks.
Frequently Asked Questions (FAQs)
Q1: Can gout go away on its own?
Acute attack. Resolves. Usually. Days to weeks. Without treatment. Anti-inflammatory medication. Accelerates. Resolution. Attacks. Prevented. Uric acid-lowering therapy. Prevention. Without uric acid control. Attacks recur. Frequently. Worsening. Time. Chronic tophaceous gout. Development. Possible. Long-term. Uric acid-lowering medications. Prevention. Lifelong. Usually. Necessary. Management. Otherwise. Progressive.
Q2: Is gout caused by eating too much red meat?
Contributing factor. Not sole cause. Genetic predisposition. Important. Red meat consumption. Elevated uric acid. Risk increased. Other purines. Seafood. Organ meats. Alcohol. Fructose. Factors. Contributing. Weight obesity. Hypertension. Chronic kidney disease. Risk factors. Major. Diet. Modifiable. Important. But genetics. Kidney function. Metabolic factors. Also critical. Multifactorial. Gout. Complex etiology.
Q3: Will I have gout attacks forever?
Not if. Uric acid-lowering therapy. Maintained. Serum uric acid. Less than 6 mg/dL. Target. Attacks. Prevention. Possible. Medication. Lifelong. Usually necessary. If stopped. Uric acid rises. Attacks. Recur. Commitment. Indefinite. Therapy. Essential. Prevention. Complications. Chronic tophaceous gout. Joint damage. Permanent. Prevention. Early intervention. Critical.
Q4: Can gout affect other joints besides the big toe?
Yes. Big toe. Podagra. Most common. First attack. 50 percent. Other joints. Ankle. Knee. Wrist. Hand. Fingers. Elbow. Shoulder. Possible. Less common initially. Later attacks. Polyarticular. Multiple joints. Affected. Simultaneously. Possible. More severe. Chronic gout. Polyarticular. Common. Tophi. Multiple locations. Subcutaneous. Visible. Deformities. Progressive. Joint damage. Widespread.
Q5: Do I need to take uric acid-lowering medication forever?
Likely. Gout. Chronic condition. Uric acid elevation. Persistent. Genetic. Lifelong treatment. Usually. Necessary. If stopped. Uric acid rises. Gout attacks. Recur. Commitment. Indefinite. Therapy. Expected. Without medication. Progressive disease. Chronic tophaceous gout. Permanent damage. Risk. Prevention. Priority. Long-term commitment. Important.
Key Takeaways
Gout is crystal arthritis. Monosodium urate crystals. Joint inflammation. Acute attacks. Extremely painful. Affects approximately 1 to 3 percent. Population. Approximately 8 to 10 million Americans. Most common inflammatory arthritis. Men. Purine metabolism. Adenosine. Inosine. Hypoxanthine. Xanthine. Uric acid. Sequential degradation. Xanthine oxidase. Final enzyme. Humans. Cannot further metabolize. Uric acid. Circulates. Blood. Kidney filtered. Excreted urine. Hyperuricemia. Serum uric acid. Greater than 6.8 mg/dL. Saturation point. Above. Crystals precipitate. Monosodium urate. Needle-shaped. Joint fluid. Acute attack. Inflammation. Triggered. Neutrophil infiltration. Phagocytosis. Crystals. Activation. Complement. NLRP3 inflammasome. Pro-inflammatory cytokines. TNF-alpha. IL-1. IL-6. Production. Pain. Swelling. Redness. Warmth. Onset. Sudden. Night. Early morning. Peak. Hours. Resolving. Days to weeks. Without treatment. Anti-inflammatory medication. Accelerates. Factors. Hyperuricemia promoting. Increased purine production. Diet. High-purine foods. Alcohol especially beer. Cell turnover. Leukemia. Chemotherapy. Reduced excretion. Chronic kidney disease. Medications. Diuretics. Low-dose aspirin. Genetic. URAT1. GLUT9. Urate transporter genes. Variation. Susceptibility. Risk factors. Obesity. Hypertension. Chronic kidney disease. Metabolic syndrome. Male. Age. Alcohol consumption. Purine-rich diet. Triggers. Acute attack. Alcohol consumption. Purine-rich meal. Dehydration. Strenuous exercise. Joint trauma. Surgery. Acute illness. Medication initiation. Diagnosis. Synovial fluid analysis. Arthrocentesis. Monosodium urate crystals. Identification. Polarized microscopy. Definitive. Gold standard. Serum uric acid. Tested. Baseline assessment. May be normal during acute attack. Management. Acute attacks. NSAIDs. First-line. Indomethacin. Naproxen. Ibuprofen. Colchicine. Low-dose. Glucocorticoids. Oral or intra-articular. Rest. Ice. Elevation. Joint. Chronic prevention. Uric acid-lowering therapy. Allopurinol. First-line. Xanthine oxidase inhibitor. Febuxostat. Alternative. Probenecid. Uricosuric agent. Pegloticase. Severe refractory. Target. Serum uric acid. Less than 6 mg/dL. Prophylaxis. Colchicine. NSAIDs. Low-dose glucocorticoids. Prevention. Attack initial therapy. Lifestyle modifications. Weight loss. Diet. Purine reduction. Alcohol elimination. Hydration. Adequate fluid intake. Exercise. Regular. Outcomes. Acute attack. Excellent. Anti-inflammatory medication. Relief. Days typically. Chronic prevention. Excellent. Uric acid-lowering therapy. Attacks prevention. Possible. Joint damage prevention. Long-term. Medication adherence. Essential. Gout—crystal arthritis—extremely painful—preventable—lifestyle modification and medication essential—prevents chronic tophaceous gout and permanent joint damage.
References
- World Health Organization (WHO). “Gout: Diagnosis and Management.” Retrieved from https://www.who.int/
- American College of Rheumatology. “Gout Clinical Guidelines.” Retrieved from https://www.rheumatology.org/
- European League Against Rheumatism. “EULAR Gout Guidelines.” Retrieved from https://www.eular.org/
- Mayo Clinic. “Gout: Diagnosis and Treatment.” Retrieved from https://www.mayoclinic.org/
- Cleveland Clinic. “Gout: Complete Information and Management.” Retrieved from https://my.clevelandclinic.org/
- National Institutes of Health. “Gout and Uric Acid.” Retrieved from https://www.nih.gov/
Related Articles on ObserverVoice.com
Explore more health and science topics on our platform:
- Purine Metabolism: Understanding Uric Acid Production
- Crystal Arthritis: Understanding Gout and Pseudogout
- Inflammatory Arthritis: Understanding Joint Inflammation
- Kidney Function: Understanding Uric Acid Excretion
- Hyperuricemia: Understanding High Uric Acid Levels
- Rheumatologic Disorders: Understanding Joint Diseases
Disclaimer
This article provides educational information adapted from publicly available health sources including WHO materials. This content is for informational and educational purposes only and does not constitute medical advice, diagnosis, or treatment recommendations. [ObserverVoice.com] is a news and information platform—not a healthcare provider. If you experience sudden severe joint pain, particularly in the big toe or foot, with swelling, redness, and warmth, consult qualified rheumatologists or primary care physicians for evaluation. Gout diagnosis requires synovial fluid analysis with identification of monosodium urate crystals under polarized microscopy. Acute gout attacks respond well to anti-inflammatory medications including NSAIDs, colchicine, or glucocorticoids. Chronic prevention requires uric acid-lowering therapy (allopurinol or alternatives) targeting serum uric acid below 6 mg/dL. Lifestyle modifications including weight loss, dietary purine reduction, alcohol elimination, and adequate hydration are critical for prevention. With appropriate acute and chronic management, gout attacks preventable and permanent joint damage avoidable. Always seek guidance from licensed healthcare specialists for gout diagnosis and long-term management.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.
Follow Us on Twitter, Instagram, Facebook, & LinkedIn