
Pneumonia: The Infectious Lung Disease Killing 740,000 Children Yearly
Why This Preventable Illness Remains the Leading Killer of Young Children
Three-month-old Fatima lay gasping for breath in her grandmother’s arms in a rural health clinic in northern Nigeria. Her tiny chest heaved rapidly, pulling inward with each labored breath. Her lips had turned blue from lack of oxygen, and her body temperature soared at 40°C (104°F). “She’s been coughing for three days,” Fatima’s grandmother explained desperately to the nurse. “At first, we thought it was just a cold. But last night she started breathing so fast, making grunting sounds, and refusing to feed. This morning, she could barely breathe at all.”
The nurse immediately recognized the danger signs—rapid breathing, chest indrawing, inability to feed, and cyanosis (blue discoloration from oxygen deprivation)—indicating severe pneumonia. Fatima needed urgent oxygen therapy, injectable antibiotics, and close monitoring. Without immediate treatment, she could die within hours. Yet the clinic had no oxygen supply, the nearest hospital with pediatric intensive care was 80 kilometers away over terrible roads, and Fatima’s family had no transportation or money for ambulance services.
Fatima represents one of millions of children facing pneumonia’s deadly threat each year. Her story illustrates both how preventable and treatable pneumonia is, yet how barriers to healthcare allow this disease to kill hundreds of thousands of children who should survive.
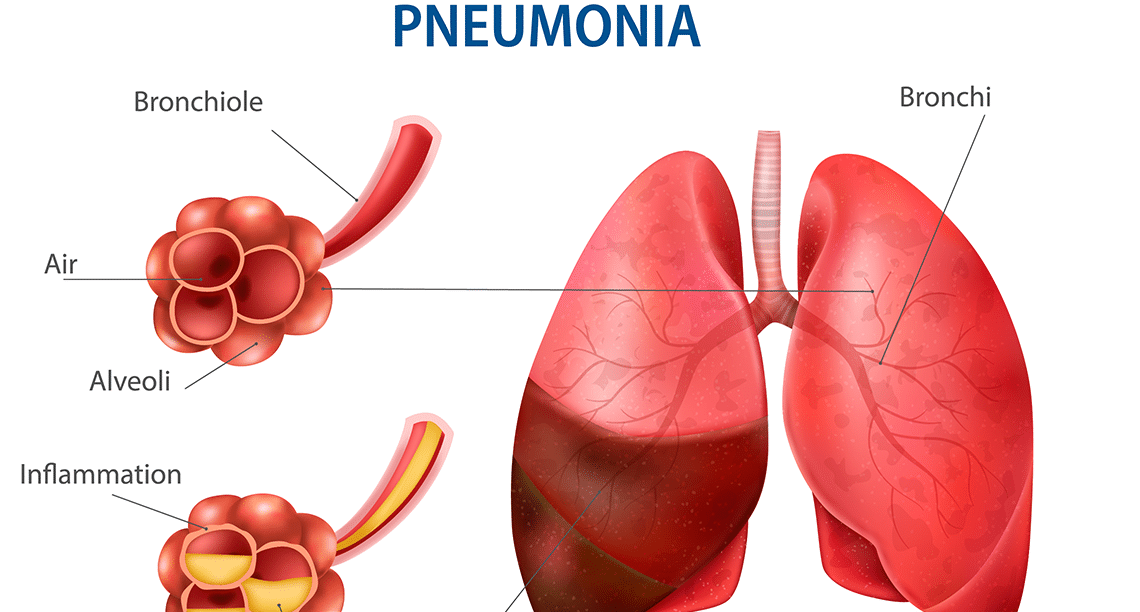
According to the World Health Organization, pneumonia is a form of acute respiratory infection that affects the lungs, causing inflammation of the air sacs (alveoli) that fill with fluid or pus, making breathing difficult and limiting oxygen intake. Pneumonia can be caused by viruses, bacteria, or fungi, though bacterial pneumonia is most common and most deadly in young children. Globally, pneumonia kills approximately 740,000 children under five years old annually—more than malaria, measles, and diarrhea combined—making it the single leading infectious cause of death in young children. Nearly all these deaths occur in low and middle-income countries. Yet most pneumonia deaths are preventable through vaccination, adequate nutrition, and addressing environmental risk factors, while most cases are treatable with inexpensive antibiotics costing less than $1.
Understanding Pneumonia
Pneumonia occurs when infection causes inflammation in the lungs’ tiny air sacs (alveoli). Normally, alveoli fill with air during breathing, allowing oxygen to pass into the bloodstream and carbon dioxide to be expelled. When pneumonia develops, alveoli fill with fluid and pus instead of air, making breathing difficult and preventing adequate oxygen from reaching the blood. This oxygen deprivation, if severe, can damage organs and cause death.
Multiple pathogens cause pneumonia. Bacteria including Streptococcus pneumoniae (the most common bacterial cause in children), Haemophilus influenzae type b (Hib), and Staphylococcus aureus account for most severe pneumonia requiring hospitalization. Viruses including respiratory syncytial virus (RSV, the leading cause of viral pneumonia in infants), influenza virus, and SARS-CoV-2 (COVID-19) can cause pneumonia, particularly in young children and elderly people. Fungi cause pneumonia primarily in people with weakened immune systems.
Pneumonia spreads through respiratory droplets when infected people cough or sneeze, direct contact with contaminated surfaces followed by touching mouth or nose, and aspiration of bacteria from mouth or nose into lungs. Young children, elderly people, and those with weakened immune systems face highest pneumonia risks.
Symptoms vary by age and pathogen but commonly include cough (may be dry or produce phlegm), rapid or difficult breathing, chest pain when breathing or coughing, fever, chills, and sweating. In young children, especially infants, specific danger signs include very fast breathing (60+ breaths per minute in infants under 2 months, 50+ in ages 2-12 months, 40+ in ages 1-5 years), chest indrawing (chest pulling inward with each breath), grunting sounds, inability to feed or drink, lethargy or unconsciousness, and blue discoloration of lips or skin indicating oxygen deprivation.
Like newborn health challenges broadly, pneumonia disproportionately kills the most vulnerable—young infants whose immune systems haven’t fully developed.
The Devastating Global Burden
Pneumonia’s global burden is staggering yet often overlooked. Approximately 740,000 children under five die from pneumonia annually—accounting for about 14% of all deaths in this age group. Additionally, pneumonia kills approximately 2.5 million people of all ages yearly. Beyond deaths, pneumonia causes approximately 120 million episodes of illness annually in children under five, requiring enormous healthcare resources.
The burden concentrates overwhelmingly in low and middle-income countries, particularly South Asia and sub-Saharan Africa, which account for over 60% of childhood pneumonia deaths. Within countries, pneumonia disproportionately affects poor families, rural populations, and marginalized communities with limited healthcare access. Several factors create this devastating burden.
Malnutrition weakens immune systems, making children more susceptible to pneumonia and less able to fight infections. Malnourished children have pneumonia death rates 2-3 times higher than well-nourished children. Lack of exclusive breastfeeding in the first six months deprives infants of antibodies and immune protection breast milk provides. Indoor air pollution from cooking with solid fuels (wood, charcoal, dung) exposes children to harmful smoke damaging lungs and increasing pneumonia risk—affecting approximately 3 billion people globally.
Overcrowding facilitates pneumonia transmission in households, childcare settings, and communities. Inadequate vaccination coverage leaves children vulnerable to vaccine-preventable pneumonia causes including Streptococcus pneumoniae (pneumococcal vaccine) and Haemophilus influenzae type b (Hib vaccine). Limited healthcare access means children don’t receive timely diagnosis and treatment—many die at home without ever seeing a healthcare worker.
Like maternal mortality and malnutrition, pneumonia deaths concentrate among populations with least access to prevention and treatment interventions.
Prevention: Vaccines and Beyond
Pneumonia prevention requires comprehensive approaches addressing multiple risk factors. Vaccination provides powerful protection against major pneumonia causes. Pneumococcal conjugate vaccine (PCV) protects against Streptococcus pneumoniae, the leading bacterial cause of severe pneumonia. Countries introducing PCV have seen pneumonia cases drop by 25-40%. Hib vaccine prevents pneumonia from Haemophilus influenzae type b. Measles vaccine prevents measles-related pneumonia complications. Pertussis (whooping cough) vaccine prevents pneumonia in infants. Influenza vaccine reduces flu-related pneumonia.
Adequate nutrition strengthens immune systems enabling children to fight infections. Exclusive breastfeeding for the first six months provides antibodies and immune protection. Vitamin A supplementation reduces pneumonia severity and death in malnourished children. Zinc supplementation supports immune function and reduces respiratory infection rates.
Reducing indoor air pollution through improved cookstoves or cleaner fuels (LPG, electricity), better ventilation in homes, and reducing environmental tobacco smoke exposure all decrease pneumonia risk. Adequate handwashing with soap reduces transmission of pneumonia-causing pathogens. Preventing HIV infection reduces pneumonia vulnerability—HIV-infected children have 5-6 times higher pneumonia risk.
Like preventing obesity and noncommunicable diseases, pneumonia prevention requires addressing multiple risk factors simultaneously.
Treatment: Simple but Time-Critical
Pneumonia treatment depends on severity and causative organism. Mild pneumonia in children can often be treated at home with oral antibiotics—typically amoxicillin for 3-5 days. This costs less than $1 for a full treatment course and cures most bacterial pneumonia if started early. Parents must ensure children complete the full antibiotic course even if symptoms improve, provide adequate fluids to prevent dehydration, and monitor for warning signs requiring medical attention.
Severe pneumonia requires hospitalization for injectable antibiotics (ampicillin plus gentamicin typically), oxygen therapy for children with low blood oxygen, intravenous fluids if unable to drink, and close monitoring for complications. Very severe pneumonia may require intensive care with mechanical ventilation.
The challenge is ensuring timely access to appropriate treatment. Community health workers trained to recognize pneumonia danger signs and provide appropriate antibiotics prevent many deaths in areas lacking health facilities. Pulse oximeters—simple devices measuring blood oxygen—help identify children needing oxygen therapy. Ensuring oxygen availability at health facilities saves lives—yet many facilities lack functioning oxygen supplies as discussed in medical oxygen access challenges.
Integrated management of childhood illness (IMCI) protocols train healthcare workers to recognize and treat pneumonia alongside other common childhood illnesses, improving outcomes. Like ensuring patient safety, effective pneumonia treatment requires functioning health systems with trained workers, essential medicines, and basic equipment.
Special Populations
Certain groups face particularly high pneumonia risks requiring targeted interventions. Newborns and young infants under two months have immature immune systems and atypical pneumonia symptoms making diagnosis challenging. They require specialized care and close monitoring. HIV-infected children have dramatically elevated pneumonia risk and mortality, requiring prophylactic antibiotics (cotrimoxazole) and antiretroviral therapy.
Malnourished children experience more severe disease and higher death rates, needing nutritional rehabilitation alongside pneumonia treatment. Children with underlying conditions including congenital heart disease, chronic lung disease, or immune deficiencies require specialized care. Elderly people, particularly those with chronic diseases, face increased pneumonia risk and complications requiring vaccination and prompt treatment.
Fatima’s Outcome
Fatima’s story had a fortunate ending. A passing physician traveling through the area happened to stop at the clinic, recognized Fatima’s critical condition, and arranged emergency transport to the district hospital in his personal vehicle. At the hospital, Fatima received oxygen therapy, injectable antibiotics, and intensive nursing care. After five days, she recovered sufficiently to go home.
“Fatima was incredibly lucky,” the physician, Dr. Ibrahim, reflected. “Most children in her situation die before reaching advanced care. She survived because of coincidence—I happened to be there with a vehicle. This shouldn’t require luck. Every child with pneumonia deserves timely access to oxygen, antibiotics, and skilled care.”
Following Fatima’s near-death experience, Dr. Ibrahim advocated with district health officials to equip rural clinics with oxygen concentrators, pulse oximeters, and essential medicines. He trained community health workers to recognize pneumonia danger signs and provide appropriate treatment or referral.
“Pneumonia kills 740,000 children annually—more than any other infectious disease,” Dr. Ibrahim emphasizes. “Yet we know how to prevent and treat it. Vaccines prevent major causes. Adequate nutrition strengthens immunity. Clean cooking fuels reduce lung damage. Simple antibiotics cure most cases. Oxygen therapy saves severely ill children. What’s needed is political will to prioritize pneumonia, adequate funding for prevention and treatment programs, ensuring vaccines reach all children, training healthcare workers in pneumonia management, equipping facilities with oxygen and essential medicines, addressing malnutrition and indoor air pollution, and recognizing that children’s lives matter regardless of geography or economic status. Every child deserves to survive preventable diseases. When we ensure universal access to pneumonia prevention and treatment, we save hundreds of thousands of lives annually and demonstrate that health equity isn’t just rhetoric but achievable reality.”
Frequently Asked Questions (FAQs)
Pneumonia is lung infection causing inflammation of air sacs (alveoli) that fill with fluid or pus instead of air, making breathing difficult. Causes include bacteria (Streptococcus pneumoniae, Haemophilus influenzae type b most common in children), viruses (RSV, influenza, COVID-19), and fungi (mainly in immunocompromised people). Pneumonia spreads through respiratory droplets when infected people cough or sneeze, direct contact with contaminated surfaces then touching mouth/nose, and aspiration of bacteria from mouth/nose into lungs. Young children, elderly people, and immunocompromised individuals face highest risk. Unlike physical activity which is behavioral, pneumonia requires pathogen exposure plus susceptibility.
Common symptoms include cough (dry or with phlegm), rapid or difficult breathing, chest pain when breathing/coughing, fever, chills, and sweating. In young children, danger signs requiring immediate medical attention include very fast breathing (60+ breaths/minute in infants <2 months, 50+ in 2-12 months, 40+ in 1-5 years), chest indrawing (chest pulling inward with breaths), grunting sounds, inability to feed or drink, lethargy or unconsciousness, and blue lips/skin indicating oxygen deprivation. Seek immediate care if child shows any danger signs or if symptoms worsen despite home treatment. Early treatment dramatically improves outcomes—delayed treatment increases death risk particularly in young infants.
Yes, many pneumonia cases are preventable through: (1) Vaccination—pneumococcal vaccine, Hib vaccine, measles vaccine, pertussis vaccine, influenza vaccine preventing major causes; (2) Adequate nutrition—exclusive breastfeeding for 6 months, adequate vitamins and minerals strengthening immunity; (3) Reducing indoor air pollution—using clean cookstoves or fuels, better ventilation, avoiding tobacco smoke; (4) Good hygiene—handwashing with soap reducing pathogen transmission; (5) Preventing HIV infection—which dramatically increases pneumonia risk; (6) Avoiding overcrowding when possible. Countries implementing comprehensive prevention strategies have reduced childhood pneumonia deaths by 40-50%, demonstrating prevention effectiveness when prioritized and adequately resourced.
Treatment depends on severity: Mild pneumonia can be treated at home with oral antibiotics (usually amoxicillin for 3-5 days costing <$1), adequate fluids, rest, and monitoring for worsening. Severe pneumonia requires hospitalization for injectable antibiotics, oxygen therapy for low blood oxygen, IV fluids if unable to drink, and close monitoring. Very severe cases may need intensive care with mechanical ventilation. Key is starting treatment quickly—pneumonia can progress rapidly particularly in young infants. Most bacterial pneumonia responds well to antibiotics if started early. However, treatment access remains inadequate in many low-income countries where children die at home without ever receiving antibiotics or oxygen.
Despite being preventable and treatable, 740,000 children under five die from pneumonia annually because: (1) Inadequate vaccination coverage—many children don’t receive pneumococcal and Hib vaccines; (2) Malnutrition weakening immunity—malnourished children have 2-3 times higher pneumonia death rates; (3) Indoor air pollution exposure—3 billion people cook with polluting solid fuels; (4) Limited healthcare access—many children live far from facilities or families cannot afford care; (5) Lack of oxygen—many health facilities lack functioning oxygen supplies; (6) Delayed care-seeking—parents don’t recognize danger signs requiring immediate treatment; (7) Weak health systems—insufficient healthcare workers, medicines, equipment; (8) Low priority—pneumonia receives less funding and attention than other diseases despite killing more children. Addressing these requires political commitment and adequate resources.
References
- World Health Organization. (2024). Pneumonia. Retrieved from https://www.who.int/health-topics/pneumonia
- World Health Organization. (2022). Pneumonia – Fact Sheet. Retrieved from https://www.who.int/news-room/fact-sheets/detail/pneumonia
- UNICEF. (2024). Pneumonia in Children. Retrieved from https://data.unicef.org/topic/child-health/pneumonia/
- Observer Voice. Newborn Health: Protecting Babies in Their First 28 Days. Retrieved from https://observervoice.com/newborn-health-protecting-babies-first-28-days/
- Observer Voice. Maternal Health: Protecting Mothers and Saving Lives. Retrieved from https://observervoice.com/maternal-health-protecting-mothers-saving-lives/
Disclaimer: This article is an adaptation of publicly available information from WHO’s Pneumonia
health topic page (WHO, Geneva. Licence: CC BYNC-SA 3.0 IGO). WHO is not responsible for the
content or accuracy of this adaptation. This content is for informational and educational purposes
only and does not constitute medical advice. ObserverVoice.com is a news and information platform
— not a healthcare provider.
Observer Voice is the one stop site for National, International news, Sports, Editor’s Choice, Art/culture contents, Quotes and much more. We also cover historical contents. Historical contents includes World History, Indian History, and what happened today. The website also covers Entertainment across the India and World.